

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The use of carbamazepine (CBZ), a common medication employed for seizure prophylaxis and multiple other neurologically based disorders, has been confirmed to be associated with severe cutaneous adverse drug reactions (SCARs) such as Stevens-Johnson Syndrome (SJS), toxic epidermal necrolysis (TEN), and drug-induced hypersensitivity syndrome with rash, eosinophilia and systemic symptoms (DRESS). Data from the medical literature suggest a strong genetic predisposition to CBZ-induced adverse events in certain Asian populations possessing the HLA-B*1502 allele [1, 2]. For example, for an association between HLA-B*1502 and CBZ-induced SCARs in the Han Chinese, there is a 100% sensitivity and 97% specificity, with a 7.7% positive predictive value and 100% negative predictive value for CBZ-induced rash, with an odds ratio (OR) of 2,504 (95% confidence interval [CI], 126-49,522) [3, 4]. These findings have been replicated in extended cohorts of subjects of Chinese descent originating from separate geographic areas of China [5, 6, 7, 8] (including Hong Kong [9]). In addition, Tassaneeyakul et al. [10] reported similar results in Thai patients, with possession of HLA-B*1502 conferring an OR of 54.76 (95% CI, 14.62-205.13) for CBZ-induced SJS/TEN. In other countries in Asia, including India [11], Malaysia [12] and Singapore [13, 14], CBZ is also a known cause of SJS/TEN. In contrast, such an association has not been demonstrated in Japanese [15] or Korean populations [4, 16, 17].
The risk of CBZ-induced SJS/TEN has not yet been determined in Vietnam, but with a documented 13.5% of people in Vietnam possessing the HLA-B*1502 allele [18], Vietnamese are probably at a high risk for CBZ-induced SCARs. In Vietnam, CBZ is utilized for epilepsy, trigeminal neuralgia, sleep disorders and various other neurologically based disorders (headache and muscular tics). It is not known whether the high incidence of SJS/TEN is secondary to the widespread use of CBZ or due to a high incidence of adverse effects to the drug CBZ. It is important to determine this risk since hypersensitivity reactions to CBZ are often life-threatening and result in significant morbidity from overlapping SJS, TEN and DRESS [19, 20]. If an association between HLA and CBZ hypersensitivity exists, a preventive program of HLA screening before administering CBZ, similar to programs in Taiwan [21] and in the United States [22], may reduce CBZ-induced SCARs morbidity and mortality in Vietnamese patients. A case-controlled study was therefore designed to determine the frequency of HLA-B*1502 in SCARs patients at a large teaching hospital in Hanoi-Bach Mai Hospital, Vietnam.
MATERIALS AND METHODS
Subjects
The study was conducted at the Center of Allergology and Clinical Immunology, Bach Mai Hospital between 2011 and 2013. There were a total of 63 participants divided into two groups (38 patients with SCARs and 25 controls). A survey instrument, focused on the history of the presenting illness, ethnicity, family history, medication usage, past medical history, any history of drug allergy and rashes, review of symptoms and physical examination, was developed. Severity-of-illness score for toxic epidermal necrolysis (SCORTEN) was applied for severity assessment [23]. SCORTEN has been defined as seven criteria including age (>40 years), heart rate (>120 beats/min), presence of malignancy, skin detachment (>10% body surface area [BSA]), serum urea level (>10 mmol/L), serum bicarbonate level (<20 mmol/L), and serum glucose level (>14 mmol/L). Maximum severity score is 7. All patients had their diagnosis of CBZ-induced SJS/TENS/DRESS confirmed by either a dermatologist or an allergologist based on the clinical morphology of the "rash" according to Roujeau [24]. Medication-induced rash was considered to have occurred when indicated by the evaluation above, when the symptoms commenced within the first 2 months of exposure to the drug and when those symptoms resolved upon withdrawal of the drug. Challenge, either blind or open, is unethical and potentially fatal. RegiSCAR inclusion and exclusion criteria were applied in this study as below. As all patients seen with drug-induced SCARs were taking CBZ.
Inclusion criteria
For SJS/TEN
CBZ was the culprit medication (established by ruling out comedication within 2 months).
Inpatients.
Widespread exanthema and more than 1% BSA skin detachment; blister formation, not acral involvement alone, with or without mucous membrane erosions.
SJS was defined as less than 10% of BSA skin detachment, ulceration in more than two natural cavities.
TEN was defined as more than 30% of BSA skin detachment and/or the presence of Nikolsky's sign.
For DRESS
CBZ was the culprit medication (established by ruling out comedication within 2 months.
Acute onset of skin rash with fever over 38℃.
Enlarged lymph nodes.
Involvement of at least one internal organ.
Eosinophilia >10% or >700/µL, atypical lymphocytes, lymphopenia < 4,000, lymphocytosis, thrombocytopenia.
All patients were fully informed as to the conduct and purposes of the study and signed a consent form.
Exclusion criteria
Patients from the same hospital as the SJS/TEN/DRESS patients who had used CBZ for more than 4 months without evidence of any cutaneous reactions were recruited as controls after signing an informed consent form (controls were recruited from the Neurology and Outpatient Departments at Bach Mai Hospital).
Calculation of skin lesion and detachment areas were based on burn area estimation (Lund-Browder formula) [25]. Index-day was defined as the period from the first day of taking CBZ to the day of onset of SCAR symptoms and signs.
Genetic analysis
Blood spot cards were used to collect the blood samples from the patients. The blood spot was required to air dry for several minutes before it was placed in an envelope for transport to the laboratory. The back of the blood spot card and its envelope were labelled with the donor's code, date and time of collection. Genomic DNA was isolated using the QIAamp DNA purification system (Qiagen, Doncaster, VIC, Australia). The combination of polymerase chain reaction and sequence-specific oligonucleotide probes with the Luminex 100xMAP flow cytometry dual laser system was then used to quantitate fluorescently labelled oligonucleotides attached to colour-coded microbeads (Sonic Clinical Institute, Sydney, NSW, Australia).
Statistical analysis
The data from the 38 subjects and 25 controls recruited into the study were used to determine statistically significant differences between groups for their clinical characteristics and HLA genotypes by using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). The OR for the possession of certain HLA alleles and the development of SCARs was determined. A p-value < 0.05 was set as the level of significance.
RESULTS
Clinical characteristics
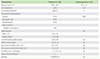
The patient demographic data are shown in Table 1. Our cohort consisted of 38 patients comprising 20 SJS (52.6%), 7 TEN (18.4%), 8 overlap syndrome (21.1%), and 3 DRESS (7.9%). The mean age was 40.6 ± 18.7 years and a slight male preponderance was noted (male:female = 20:18). The controls (n = 25) had a mean age of 22.4 ± 13.1 years and a slight male preponderance was observed (male:female = 13:12). Involved skin lesion areas in SCARs-affected patients was 62.1% ± 24.1% of BSA, skin detachment areas of 12.3% ± 12.9% of BSA, SCORTEN scores exhibited a mean of 1.1 ± 1.0 (range, 1 to 4) and Index-days were 14.2 ± 8.3 days (median, 12.5 days). Indications for CBZ were epilepsy (34.2%), neuropathic pain (42.1%), mental disorders (18.4%) and other conditions (headache and muscular tics) (5.3%).
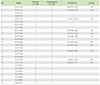
In our study, we also found that three patients who developed SCARs with CBZ therapy had a history of prior rashes induced by phenytoin and phenobarbital in a total of 4 exposures (60%) (Table 2).
Eleven patients with SCARs had a history of herpes infection, whilst only 1 CBZ tolerant patient had a history of herpes infection (OR, 9.78; 95% CI, 1.17-81.43; p = 0.02).
The associations between HLA-B and CBZ-induced SCARs
When we analysed for an association between HLA-B*1502 and specific phenotypes, a strong association between HLA B*1502 and bullous skin reactions such as SJS/TEN and overlap was confirmed with an OR of 33.78 (95% CI, 7.55-151.03; p < 0.0001), sensitivity 91.4%, specificity 76.0%, positive predictive value 84.2% and negative predictive value 86.4%. We did not, however, observe any correlation between the presence of this allele and CBZ-induced non-bullous skin reactions (DRESS), (OR, 6.33; 95% CI, 0.48-82.74; p = 0.1592).
Overall, the HLA-B*1502 allele was detected in 34/38 patients (89.5%) with CBZ-induced SCARs, whilst this allele was found in only 6/25 controls (24.0%). The OR for HLA-B*1502 positivity was 26.9 (95% CI, 6.7-107.4; p < 0.001), sensitivity 89.5%, specificity 76.0%, positive predictive value 85% and negative predictive value 82.6% (Tables 3, 4).
By extending our investigation into examining for other HLA-B alleles, we found that HLA-B*4601 was detected more frequently in controls, with 9 of 25 controls possessing HLA-B*4601 versus 5 of 38 of our SCARs patients (OR, 0.27; 95% CI, 0.08-0.94; p = 0.03) (Table 5).
DISCUSSION
In this study, we found that 34/38 SCARs patients (89.5%) possessed the HLA-B*1502 allele in comparison with 6/25 controls (24%) (OR, 26.92; 95% CI, 6.74-107.43; p <0.001). HLA-B*1502 was strongly confirmed as conferring genetic susceptibility to CBZ-induced bullous skin reactions such as SJS/TEN and overlap with OR of 33.78 (95% CI, 7.55-151.03) versus nonbullous skin reactions with OR of 6.33 (95% CI, 0.48-82.74) in Vietnamese. Although HLA-B*1502 was detected in 2 of 3 DRESS patients, this prevalence was not significantly different to its prevalence in the control group. This finding is similar to those in a number of previous studies in Asians with different ancestries such as Han Chinese [3, 4, 6, 7, 8, 9], Thais [4, 10, 27], Malays [4, 12], Indians [11] and Singaporeans [4, 13]. Vietnam is similar to other countries in Asia then, in that the presence of HLA-B*1502 strongly predisposes to the development of immunologically-induced bullous skin rashes due to CBZ hypersensitivity. In our study, however, we observed a much higher prevalence of HLA-B*1502 in the CBZ-tolerant group compared with that observed in any other previous study (11.9% [10] and 18% [27] in two Thai studies, 8% in central Han Chinese [7] and 13.75% in southern Chinese Hans [6]. This finding is likely to be due to the high prevalence overall of HLA-B*1502 in our population (13.5%), although the smaller number of controls compared with our patient group might be considered as a limitation of our study and the inclusion of a larger number of controls in any future study may clarify the significance of our initial observation.
In regard to HLA-B*4601, the prevalence of this variant is significantly different between patients and controls (OR, 0.27; 95% CI, 0.08-0.94; p = 0.03), being found more commonly in the controls. This suggests that the presence of this allele may be protective against the development of CBZ-induced SCARs in Vietnamese. In keeping with our finding, Alfirevic et al. [28] noted in Caucasians that the presence of the HLA-B*0702 allele appears to be protective in terms of developing CBZ hypersensitivity while HLA-B*4001 and HLA-A*2402 have been demonstrated to be protective markers in Asian populations [29]. However, HLA-B*4601 is the second commonest allele (11.5%) among HLA-B genes in the Vietnamese population [18]. It follows therefore that the lower prevalence of HLA-B*1502 in the controls would be likely compensated for by a higher prevalence of HLA-B*4601. Therefore, the supposition that the presence of the HLA-B*4601 allele might be protective needs to be confirmed in a study with a larger number of controls.
We did not find an association between the presence of HLA-B*1511 and the development of SJS/TEN, as has been reported in other Asians [26]. In addition, this allele was not found in the study of 170 Kinh Vietnamese conducted by Hoa et al. [18]. Thus it seems reasonable to conclude that HLA-B*1511 is not a genetic risk factor for CBZ-induced SCARs in Vietnamese.
Cross-reactivity exists frequently between CBZ, phenytoin and phenobarbital and both phenytoin and phenobarbital are known to cause SCARs in their own right [30, 31, 32, 33, 34]. In their study, Wang et al. [33] indicated that 52.9% of patients who had previously experienced rashes with CBZ, also reacted to phenytoin while 69.2% of patients with previous phenytoin reactions also had rashes with CBZ. Seitz et al. [31] postulated that cross-reactivity among aromatic anticonvulsants may be even higher than 80%. This is in keeping with our findings that three patients who developed SCARs with CBZ therapy had a history of prior rashes induced by phenytoin and phenobarbital in a total of 4 exposures (60%) (Table 2). This finding emphasizes the cross-reactivity risks for patients treated with any drug in the aromatic anticonvulsant group and consequently, the use of cross-reactive drugs should be avoided in our population. Moreover, work by Hu et al. [35] (albeit their patients suffered mild cutaneous reactions) indicates that patients with HLA-B*1502 should also avoid newer anticonvulsants such as oxcarbazepine. Conversely, when our controls tolerated CBZ, they also tolerated other anticonvulsants such as phenytoin, phenobarbital, oxcarbazepine and sodium valproate. Our finding also stressed that no SCARs-induced CBZ patient (0/4) had previous reactions to nonaromatic anticonvulsant drugs such as valproate, topiramate or gapabentin. Our clinical recommendation is that patients who have previously developed rashes to CBZ should be treated with nonaromatic anticonvulsant agents.
The age range of those affected by SCARs may reflect the age range wherein CBZ use is more likely rather than implying that the age of the patient predisposes to the development of these conditions; however, our data suggest that there is an increased risk of developing SCARs in middle age compared to the first few decades of life (mean age 40.6 ± 18.7 in the patient group vs. 22.4 ± 13.1 in the control group). In keeping with our finding, Seitz et al. [31] reported that the mean age of 36 patients with anticon-vulsant hypersensitivity was 59 years (range, 13-92 years) and the mean age in 24 patients reported by Kim et al. [16] was 52.1 ± 15.1 years. Alvestad et al. [36] also concluded that the number of CBZ-induced skin rashes significantly increased with age (6% [10/172] in the group under 16 years, 12% [33/270] in those aged from 16-49 years and 19% [10/53] in those aged over 50 years, p = 0.012). Generally, however, it seems to be that adverse drug reactions occurring in inpatients are more prevalent in the older age group compared with younger patients [37]. Irrespective of age, possession of the HLA-B*1502 genotype is strongly associated with the occurrence of SCARs in our patients.
Our data showed a slight male preponderance in the group with SCARs (male:female = 20:18). This finding was also noted by Kim et al. [16] and Zhang et al. [8]. However, generally, in studies based on larger sample sizes, CBZ-induced skin rashes were significantly increased in females. In their review of 137 Han Chinese patients with anticonvulsant hypersensitivity, Wang et al. [33] indicated that development of a rash was nearly twice as frequent in females (OR,1.84; 95% CI, 1.32-2.60; p < 0.001). Further, Alvestad et al. [36] reported that CBZ-induced rash occurred more commonly in females (19% vs. 8%, respectively, p < 0.001) and they postulated that this finding results from the impact of sex hormones on T-cell populations as CBZ hypersensitivity is an immunologically T-cell-mediated reaction. This female preponderance remains to be confirmed across the clinical spectrum of CBZ hypersensitivity.
An association between SCARs and herpes infection has been described previously and confirmed serologically [38, 39, 40, 41]. Our data suggest an association may exist in our population with OR, 9.78 (95% CI, 1.17-81.43; p = 0.02) when comparing patients and controls. Historically, a number of patients had suffered from herpes infection. Some of them were tested for herpes simplex virus type 1 (HSV1) and herpes simplex virus type 2 (HSV2) and were IgG positive. Oskay et al. [39] concluded in their study that anticonvulsant hypersensitivity was accompanied by serological evidence of human herpes virus (HHV-6 and HHV-7) infection and reactivation but had no significant association with HSV infection. Unfortunately, in our hospital we are not able to identify the human herpes viruses type 6 and 7 and therefore cannot confirm our clinical findings serologically. Most studies, however, suggest human herpes virus type 6 is the likely culprit of anticonvulsant hypersensitivity syndrome [40].
Lastly, the majority of our patients developed their first symptoms early during therapy with an index-day median of 12.5 days (range, 2-49 days). Chong et al. [13] reported that the median time span in their group of CBZ-induced SJS/TEN sufferers was 12 days (range, 11-13 days) and 16 days (range, 10-37 days) in DRESS patients. In our study, we observed that the first symptom appeared later at a median of 16 days (range, 15-49 days) in the three patients with DRESS compared with the group with SJS/TEN and overlap with a median of 12 days (range, 2-30 days). Studies conducted by Kim et al. [16] in Koreans and by Chong et al. [13] in Singaporeans have documented similar findings to those in our study.
In future studies, we would like to be able to clarify any association in our patients between herpes virus infection and SCARs, identify the type of herpes infection, and confirm this serologically.
Regarding the limitations of this study, we also realize that additional data will be required to determine whether gender and age play a role in susceptibility to SCARs in our population. Having an age-matched control group and expanding the control group numbers would be desirable in any future study, as these improvements might allow us to resolve whether the high prevalence of HLA-B*1502 in our controls is due to the high prevalence of this allele in the Vietnamese population in general.
HLA-A*3101, the presence of which has been associated with the development of CBZ-induced hypersensitivity reactions in Caucasians [42], was not evaluated in this study because HLA_A*3101 is quite rare in Vietnamese (2.1%) [18] and therefore the number of patients we were able to evaluate in this study precluded searching for such an association. Future studies searching for this association in larger numbers of patients will be required to determine whether there exists an association between the presence of HLA-A*3101 and the development of SCARs in Vietnamese.
In conclusion, we have demonstrated that Vietnamese patients are at greater risk of developing SCARs from anticonvulsant therapies and this finding is in keeping with studies from other Asian countries. Our study indicates that Vietnamese patients, therefore, should have their HLA genotype determined prior to be planned commencement of therapy with CBZ. As genotype confers this increased risk, our findings have implications for those of Vietnamese ethnicity living elsewhere in the world. To reduce the mortality and morbidity associated with these severe drug-induced reactions we propose that Vietnamese patients, here or overseas, have their HLA genotype determined, prior to the planned commencement of any of the aromatic anticonvulsants and if they are found to possess HLA-B*1502, they should not be treated with CBZ, phenytoin, phenobarbital or oxcarbazepine or any aromatic anticonvulsants developed in the future.



 XML Download
XML Download