

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atopic dermatitis (AD) is a chronic pruritic relapsing inflammatory skin disease with variable clinical features [1]. AD has been categorized into two types i.e. the classic IgE-mediated allergic (extrinsic form; eAD) and non-allergic (intrinsic form: iAD or atopiform dermatitis) [2]. The European Academy of Allergy and Clinical immunology nomenclature task force has proposed the term "atopic eczema/dermatitis syndrome (AEDS)" to cover the different subtypes of AD [3]. The intrinsic or non-allergic AEDS shows normal serum IgE levels, no serum specific IgE, no association with respiratory diseases and negative skin prick testing (SPT) to common aeroallergens or food allergens. Serum total IgE values less than 150 or 200 kU/L have been proposed to indicate iad [2]. The reported frequency of intrinsic AD ranged from 10 to 45% [4].
Most studies concerning the prevalence and dermatological manifestations of both types were performed in children and adult AD related to the early-onset AD extending to adult life. Fölster-Holst et al. [5] reported low prevalence of the iAD (5.4%) among 259 adult AD patients. Adult-onset AD is a subgroup of AD. Apart from the typical eczematous flexural distribution pattern of AD, this group may also have nontypical morphology and localization [6].
The purpose of this study was to compare the clinical and diagnostic features of patients with extrinsic and intrinsic type of adult-onset AD.
MATERIALS AND METHODS
This study was approved by Siriraj Institutional Review Board, Siriraj Hospital, Mahidol University, Bangkok, Thailand. We retrospectively reviewed case records of patients diagnosed as adult-onset AD who attended the skin allergy clinic, Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand from June, 2006 to May, 2008. The diagnosis of AD was made according to the criteria of Hanifin and Rajka [7] and the severity of AD in each patient was assessed using the eczema area and severity index (EASI) score [8], range of score 0-72 (mild, <6; moderate, 6-17; severe, ≥18) and the Rajka and Langeland score, range of score 0-9 (mild, 3-4; moderate, 4.5-7.5; severe, 8-9) [9]. UK working party's criteria (Williams' criteria) [10] and Millennium criteria [11] were also recorded. We used the age of 18 years as the cut-off mark to determine the adult-onset AD. Subjects who had other skin diseases that might interfere with the clinical features of AD or were unwilling to participate in the study were excluded.
Demographic data, a complete history including personal and family history of atopy, onset and activity of personal atopy, course of dermatitis, and previous treatment were reviewed. Physical examination, morphology and distribution of dermatitis were studied. Investigations included SPT using 28 allergens, serum total IgE levels determined by Nephelometry method (Dade Behring, Germany). Normal levels were less than 100 kU/L.
The intrinsic form of AD was defined by low total serum IgE levels (<200 kU/L), no specific serum IgE antibodies and/or negative SPT for common aeroallergens and/or food allergens, and the absence of associated respiratory atopic diseases [5].
SPT
The SPT is performed by placing a purified drop of antigen extract on the skin then using a hypodermic needle to gently tent the skin and puncture it in order to introduce the allergen. 0.9% saline and histamine 10 mg/mL were included as negative and positive controls, respectively. In all patients, skin reactivity was tested on the volar surface of the forearm by the trained and experienced person. The results were read at 15 min. A positive result yields a wheal at least 3 mm in diameter larger than negative control. The studied allergens included 15 food allergens (egg white, egg yolk, cow's milk, wheat, banana prawn, giant tiger prawn, giant freshwater prawn, undulated surf clam, green mussel, blue swimming crab, sea crab, snapper, cuttlefish, butterfish, mackerel) and 13 aeroallergens composed of molds (aspergillus, penicillum, cladosporium), pollens (para grass, bermuda grass, careless weed, sedge, sugar cane), house dust, mites (Dermatophagoides pteronyssinus, Dermatophagoides farinae), cat hair, dog epithelium and cockroach.
Statistical analysis
Descriptive statistics e.g. median, minimum, maximum and percentages were applied to describe demographic data, and laboratory findings. Comparison of demographic and clinical data between iAD and eAD was performed using Pearson's chi-square test or Fisher exact test for qualitative data and unpaired t-test or Mann-Whitney U test for quantitative data with and without normal distribution, respectively. An odds ratio greater than 1 indicates that the condition or event is more likely to occur in eAD and an odds ratio less than 1 indicates that the condition or event is more likely to occur in iAD. However, the significant cut-off marks were at ≥2 and ≤0.5, respectively. SPSS for Windows version 17 (SPSS, USA) performed the tests to analyze all statistical data.
RESULTS
Fifty six patients were enrolled (46 females, 10 males) with an age range of 18 to 72 years (mean 34.1 ± 11.7 years). The ages of onset ranged from 18 to 59 years (mean 29.4 ± 10.5 years). The majority of the patients developed their dermatitis within the third decade. Nine patients had negative SPT results. Among these patients, seven had serum IgE level less than 200 kU/L and had no history of atopy, so they were diagnosed as iAD.
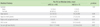
Table 1 showed demographic data of the patients. Of 56 patients with adult-onset AD, 49 (87.5%) was eAD and 7 (12.5%) was iAD. Females predominated in both groups. Elevated serum total IgE level (>200 kU/L) was detected in 37% of eAD patients. By using the Rajka and Langeland score, the severity of eAD patients in this study was mild in 20.9% of cases and moderate in 79.1% of cases. Among iAD patients, the severity was mild in 28.6% of cases and moderate in 71.4% of cases.
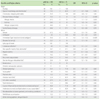
Comparison of the Hanifin and Rajka criteria between eAD and iAD is shown in Table 2. Patients with eAD frequently had flexural lichenification when compared with patients with iAD, and had a statistically significant higher percentage of personal history of atopy, especially allergic rhinitis, than those with iAD. In contrast, ichthyosis, cutaneous infection, non-specific hand and foot dermatitis, Dennie-Morgan infraorbital fold, orbital darkening, facial pallor, anterior neck folds, itch when sweating, course influenced by environment or emotional factors, intolerance to wool and lipid solvent or any coarse fabric were commonly seen in iAD when compared with eAD patients.
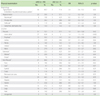
Comparison of skin lesions between eAD and iAD is shown in Table 3. Our study showed that both groups usually had typical lichenified/exudative eczematous lesions. Nummular and follicular lesions were more commonly seen in iAD group than the eAD group. Concerning the location, lesions on antecubital and popliteal area were detected more commonly in eAD (62.8% and 30.2% respectively). The most common area of involvement in patients with iAD was non-flexural area (71.4%) especially trunk and legs (57.1% each), followed by flexural area (57.1%) and extensor area (42.9%), respectively.
Our study showed that patients with eAD had positive SPT results in 95.9% of cases (food allergens, 50%; aeroallergens, 82.6%). Mites were the most commonly detected aeroallergen (69.6%), while giant tiger prawn and giant freshwater prawn were the most commonly detected food antigens (23.9%).
By using the EASI and the Rajka and Langeland score in our study in adult-onset AD population, severity of both iAD and eAD did not show a significant difference. By using the criteria other than the the Hanifin and Rajka criteria in this study, Williams' criteria had sensitivity at 81.6% and specificity at 14.3% in the diagnosis of both eAD and iAD while the Millennium criteria had sensitivity at 93.9% and specificity at 100% (Table 4).
DISCUSSION
Our study showed eAD in 87.5% and iAD in 12.5% of adult-onset AD patients. This finding correlates with previous reports in general AD patients (children and adult AD related to the earlyonset AD extending to adult life) that eAD is reported to be more predominant among AD patients [5, 12-15] while iAD has been reported in 10-45% of AD patients depending on the analysed patient population [5, 12, 14, 15]. Fölster-Holst et al. [5] reported a prevalence of iAD in adult patients that decreased from 6.8% to 5.4% after a median follow-up period of 7.5 years due to the previous iAD patients who either developed respiratory allergy or IgE-mediated sensitization. Other reports also showed similar results [12, 16]. These might explain the small number of iAD in our adult-onset AD study population.
Similar to previous studies in general AD patients which indicated that female patients were predominant in both eAD (range from 68% to 72%) and iAD (range from 60% to 90%), our study also revealed female predominance in both eAD and iAD (81.6% and 85.7%, respectively) [5, 12, 14]. In contrast, Ott et al. [14] showed males were predominant in eAD group (60%).
Total serum IgE level was reported to be associated with allergen-specific IgE status [14]. Serum IgE has been postulated to be a significant parameter for differentiation between eAD and iAD. It has been proposed that total serum IgE level below 150-200 kU/L was an indicator of iAD [2, 5]. Among our iAD patients, median of serum IgE level was 22 kU/L.
On the other hand, low total serum IgE level was also found in eAD group. Fölster-Holst et al. [5] reported that 32 of 83 of AD patients with low total serum IgE level (<200 kU/L) (39%) had allergic rhinitis and/or asthma. Among the remaining 51 patients with low total serum IgE level, 33 cases (64.7%) had serum specific IgE antibodies or positive SPT results. In our study, 17 patients had normal total serum IgE level. However, 15 patients (88.2%) had positive SPT and 11 patients (64.7%) had positive personal atopic history, so they were categorized into eAD group.
Previous reports suggested that the dermatological manifestations of eAD and iAD were indistinguishable [4]. However, Brenninkmeijer et al. [12] reported that the intrinsic form in their study had female predominance, higher frequency of the Dennie-Morgan infra-orbital folds, the later onset of the disease and milder disease severity. The features with less frequent association with intrinsic form included personal or family history of atopy, recurrent conjunctivitis, pityriasis alba, keratosis pilaris, hand and foot eczema, palmar hyperlinearity and influence of environmental or emotional factors [12].
Skin barrier function is usually assessed by transepidermal water loss and skin surface hydration. The skin barrier function was preserved in iAD but impaired in eAD [13], probably because of filaggrin gene mutation [17, 18]. Filaggrin mutations are also associated with palmar hyperlinearity which is a shared feature of AD and ichthyosis vulgaris [19]. The disturbed skin barrier allows the entry of environmental allergens into the skin and increases density of Langerhans cells in epidermis. The IgE receptors on Langerhans cells mediate the binding of environmental allergens, which trigger Th2 immune response leading to atopic inflammation [18, 20]. Akdis et al. [21] reported that eAD patients had increased expression of the high-affinity receptor for IgE in comparison with iAD patients.
In our study in adult-onset AD population, flexural lichenification, personal history of atopy, especially allergic rhinitis, or family history of atopy increased with an upward trend in eAD group when compared with the iAD group. Surprisingly, ichthyosis, non-specific hand and foot dermatitis, a course influenced by environment factors had a greater tendency to be detected in our iAD rather than eAD patients. It should be noted that we had a small number of population of the iAD group. Further study with a large number of patients should be performed.
Brenninkmeijer et al. [12] reported that iAD patients exhibited statistically significant milder disease severity than eAD by using SCORAD. However, when using EASI score, even iAD showed milder severity, but there was no statistically significant difference [12]. Fölster-Holst et al. [5] also reported that iAD patients had milder disease severity than eAD by using SCORAD. By using EASI score and Rajka and Langeland score in our study in adult-onset AD population, severity of both iAD and eAD did not show a significant difference. The Rajka and Langeland scores in most of our patients were rating as moderate severity while the severity of the disease seemed to be less severe when using the EASI scoring system. The explanation may be because the Rajka and Langeland scoring system included a retrospective self-assessment of the AD severity such as pruritus severity and history of disease remission while EASI system is a cross-sectional objective disease severity evaluation. Yang et al. [22] reported that EASI did not show a correlation with the subjective AD severity.
In conclusion, the eAD type of adult-onset AD was more common than the iAD type. Patients with eAD had more common flexural lichenification whereas the iAD group tended to have more common nonflexural area involvement. The severity of both iAD and eAD did not show a significant difference.

 XML Download
XML Download