

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
It is often presumed that apical periodontitis follows total pulp necrosis, and consequently root canal treatment is commonly performed. Periapical lesion development is usually caused by bacteria and its byproduct which irritate pulp, develop pulpitis, and result in necrosis through an irreversible process. Afterwards, apical periodontitis occurs. This phenomenon is observed as an apical radiolucency in radiographic view. However, this unusual case presents a spontaneous healing of periapical lesion, which has developed without pulp necrosis in a vital tooth, through conservative treatment.
Figures and Tables
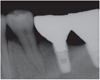
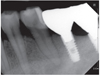
Figure 1
Preoperative periapical view and clinical photograph. (a) Periapical radiolucency on #35; (b) Cervical abrasion.
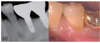
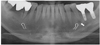
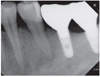
Figure 2
Preoperative panorama view. Periapical radiolucency was observed at the apex of mandibular left second premolar.





References
1. Kim IS, Kim SG, Kim YK, Kim JD. Position of the mental foramen in a Korean population: a clinical and radiographic study. Implant Dent. 2006. 15:404–411.

2. Resnick CM, Novelline RA. Cemento-osseous dysplasia, a radiological mimic of periapical dental abscess. Emerg Radiol. 2008. 15:367–374.
3. Romanos GE, Froum S, Costa-Martins S, Meitner S, Tarnow DP. Implant periapical lesions: etiology and treatment options. J Oral Implantol. 2011. 37:53–63.
4. Kovacević M, Tamarut T, Jonjić N, Braut A. The transition from pulpitis to periapical periodontitis in dogs' teeth. Aust Endod J. 2008. 34:12–18.
5. Khayat BG, Byers MR, Taylor PE, Mecifi K, Kimberly CL. Responses of nerve fibers to pulpal inflammation and periapical lesions in rat molars demonstrated by calcitonin gene-related peptide immunocytochemistry. J Endod. 1988. 14:577–587.
6. Byers MR, Taylor PE, Khayat BG, Kimberly CL. Effects of injury and inflammation on pulpal and periapical nerves. J Endod. 1990. 16:78–84.
7. Caviedes-Bucheli J, Muñoz HR, Azuero-Holguín MM, Ulate E. Neuropeptides in dental pulp: the silent protagonists. J Endod. 2008. 34:773–788.
8. Stashenko P, Teles R, D'Souza R. Periapical inflammatory responses and their modulation. Crit Rev Oral Biol Med. 1998. 9:498–521.
 XML Download
XML Download