

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
White spot lesions are defined as the enamel lesions that look chalky white and opaque. It can arise from developmental cause such as fluorosis, idiopathic cause or early caries lesion. Incipient caries, one of the white spot lesions, is the enamel caries lesion that can be clinically recognized for the first time.
White spot lesions develop as a result of a dietary carbohydrate and saliva modified bacterial infection, resulting in an imbalance between demineralization and remineralization of the enamel.1,2 And these are generally considered to be the precursor of frank enamel carious lesions.3 The white appearance is due to an optical phenomenon which is caused by mineral loss in the surface or subsurface enamel. Enamel crystal dissolution begins with subsurface demineralization, creating pores between the enamel rods. The resultant alteration of the refractive index in the affected area is then a consequence of both surface roughness and loss of surface shine and alterations in internal reflection, all resulting in greater visual enamel opacity, as porous enamel scatters more light than sound enamel.4
In regard to the prevalence of white spot lesions, it has been reported that there is a significant increase in the prevalence and severity of enamel demineralization after orthodontic treatment.3 The overall prevalence of white spot lesions amongst orthodontic patients has been reported as anywhere between 2 and 96 percent.5 Some white spot lesions may remineralize and return either to normal or at last to a visually acceptable appearance. However, white spot lesions may also persist, resulting in an aesthetically unacceptable result.3
Several techniques have been proposed to improve the appearance of white spot lesions. The common treatment strategy for white spot lesions comprises restorative procedures, improvement of reminealization using CCP-ACP containing or fluoride containing products, microabrasion, argon-laser irradiation.6,7 Recently, 'resin infiltration technique' was introduced with the development of highly-flowable resin material. The following case report describes the effect of resin infiltration technique to mask white spots that was detected after debonding of fixed orthodontic appliance and calculus removal.
Case reports
After reading and receiving all necessary explanations including the experimental rationale, the clinical procedures and possible risk, the patients were asked to sign a consent form explaining the research protocol, which was previously approved by the Ethics Committee of Pusan National University Hospital Medical Research Institute (IRB, 2010092).
1. Case 1
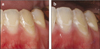
A 26-year-old female came to correct the white lesions on mandibular anterior teeth and premolars (Figures 1a, 2a, 3a). The patient's history included orthodontic treatment 10 years ago and the white spot lesions had existed since brackets were removed. Under the agreement, a decision was made to perform microabrasion with Opalustre (Ultradent Products, Inc., South Jordan, UT, USA) on the left side and resin infiltration technique with Icon (DMG, Hamburg, Germany) on the right side of mandibular teeth. The materials used are shown in Table 1.
After OpalDam (Ultradent Products, Inc.) and rubber dam were applied, microabrasion was performed on the left side first. The teeth looked chalky-whitish and the white spot lesions became more prominent than before (Figures 1b and 2b). Then resin infiltration was performed on the right side. The size of white spot lesion became smaller, however, somewhat was left (Figures 1b and 3b). Neither microabrasion nor resin infiltration technique can remove the white spot lesions completely. However, the lesions on the right side, resin infiltrated teeth, became smaller and the lesions on the left side, microabrased teeth, became more opaque. Therefore, white spot lesions on the microabrased teeth were more conspicuous after treatment.
2. Case 2
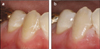
A 23-year-old female came with esthetic concern of anterior teeth (Figure 4a). Patient's history included orthodontic treatment 15 years ago. Because whitish lines on the maxillary right central incisor and white spot lesions on the maxillary left central incisor were detected (Figure 5a), fluoride varnish was applied periodically, but white spot lesions were not removed. Under the patient's agreement, a decision was made to perform microabrasion with Opalustre on maxillary right central incisor, resin infiltration technique with Icon on maxillary left central incisor and resin restoration on maxillary left lateral incisor. Whitish lines on the maxillary right central incisor which was treated by microabrasion became more whitish but the lesion on the maxillary left central incisor which was treated by resin infiltration technique looked smaller (Figures 4b and 5b). Even though some lesions are still left after treatment, resin infiltration technique seems more efficient with regard to the diminution of lesion size.
Discussion
White spot lesions are detected frequently and can be problematic for the patients with much esthetic concern. Several techniques have been proposed to improve the appearance of these white spot lesions. Among these, remineralization can be considered first for correct these white spot lesions. Because remineralization is a natural phenomenon resulting in the partial reversal of what is an early caries lesion. According to Willmote who studied the effect of fluoride and saliva after removal of fixed orthodontic appliance, the difference in percentage reduction of the white spot lesion size showed a reduction in lesion area of about a third after 12 week and a half after 26 weeks.8 However, remineralization of white spots takes a long time, and the lesions may be left to some degree. And it can inhibit the mineralization of subsurface lesions.
On the other hand, Ogaard et al. warned against treating visible white lesions on labial surfaces with concentrated fluoride agents, since this arrests the lesion (hypermineralization) and prevent complete repair.5 Especially deep lesions tend to remineralize only superficially. Consequently, arrested lesions show thick and highly mineralized surface layers.9 The underlying lesion body is still porous, however, and thus the whitish appearance often persists.10 Moreover, during remineralization stains can be incorporated into the lesion, leading to the formation of brown spots, a situation that might be judged as even more unesthetic.9 Therefore, some authors advocated allowing slow and gradual remineralization by saliva or low-concentrated fluoride agents such as fluoride mouth rinse and fluoride containing toothpaste on shallow lesion (< 60 µm), as this results in greater repair and less visible lesion.5
Enamel microabrasion was designed to improve the surface texture, remove the stains and recover remineralization. It removes superficial parts of the lesion by abrasion with a slurry of hydrochloric acid and pumice, and the enamel surface becomes smooth and glossy.10 Both chemical erosion with hydrochloric acid and mechanical abrasion with pumice simultaneously take place. Consequently, it uniformly removes up to 0.2 mm of enamel surface. According to Murphy et al. the mean reduction in white spot lesion size was 83%.11 Microabrasion can be applied for white spot lesion, fluorosis, demineralizarion after orthodontic treatment, localized hypoplasia, idiopathic hypoplasia. Donly et al. found that microabrasion re-created the outer, prism-free region and teeth became glassy and named 'abrosion effect'.12 This layer reflects or scatters the light and masks mild imperfections. However, substantial amounts of enamel often unfortunately have to be eroded to improve appearance with this technique.13
Resin infiltration technique is an alternative therapeutic approach to prevent further progression of enamel lesions. This treatment aims to occlude the microporosities within the lesion body by infiltration with low-viscosity light-curing resins that have been optimized for rapid penetration into the porous enamel.14 The resin penetrates into the lesion body, driven by capillary forces. This technique aims to create a diffusion barrier inside the lesion, not on the lesion surface. Robinson et al. reported that about 60 ± 10% of the lesion's pore volume had been occupied by resin.15 According to Kielbassa et al., resin infiltrates into subsurface lesions and produces resininfiltrated parts of the lesion.16 And the depth of resin infiltration was over 100 µm.
A positive side effect of resin infiltration is that enamel lesions lose their whitish appearance when their microporosities are filled with the resin and look similar to sound enamel. The principle of masking enamel lesions by resin infiltration is based on changes in light scattering within the lesions. Sound enamel has a refractive index (RI) of 1.62. The microporosities of enamel caries lesions are filled with either a watery medium (RI 1.33) or air (RI 1.0). The difference in refractive indices between the enamel crystals and medium inside the porosities causes light scattering that results in a whitish opaque appearance of these lesions, especially when they are desiccated.17 The microporosities of infiltrated lesions are filled with resin (RI 1.46) that, in contrast to the watery medium, cannot evaporate. Therefore, the difference in refractive indices between porosities and enamel is negligible and lesions appear similar to the surrounding sound enamel.18 As a result, this treatment may be used not only to arrest enamel lesions but also to improve the esthetic appearance of buccal white spots.
As to <Case 1> and <Case 2>, the patients had history of orthodontic treatment and the white spot lesions were detected immediately after removal of fixed orthodontic appliances. To improve the remineralization, reinforcement of oral hygiene and fluoride varnish application was tried. However, the white spot still had existed for 10 years and 15 years. Therefore, change of treatment option is needed and decision was made to perform resin infiltration technique and microabrasion which are generally known as effective methods for correction of white spot lesions. As a result of microabrasion, white spot lesions look more whitish and opaque. On the other hand, significant size reduction of white spot lesion was detected in the resin infiltrated teeth.
Unfortunately, neither microabrasion nor resin infiltration technique can remove white spot lesions completely. The reason why some lesions are left after treatment could be thought that the depth of white spot lesion is not restricted to superficial part of enamel. It is reported that 200 µm of superficial enamel is removed by microabrasion and the depth of resin infiltration is about 60 µm.19 If the depth of white spot lesion is deeper than that of microabrasion or resin infiltration technique, it could still be detected. Therefore, caution should be taken for case selection.
In the limitation of this study, the findings of the present case report showed that resin infiltration technique seems to be more effective for correction of white spot lesion and caution should be taken for case selection.




 XML Download
XML Download