

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporosis is a systemic disease of the bone and a leading cause of fractures that can result in deterioration of bone strength1). Osteoporotic hip fracture (OHF) is associated with high mortality and morbidity, and is particularly fatal in the elderly234). A large number of patients with OHF are unable to ambulate independently, and OHF can be associated with simultaneous fractures in other parts of the body5678). Consequently, effective management and adequate medication treatment of OHF are important for lowering the risk of associated fractures, mortality, and morbidity234). However, patients with osteoporotic fractures are less likely to be evaluated and managed for osteoporosis by physicians who are responsible for treating symptomatic fractures910). A systematic review indicated that bone mineral density (BMD) scans are performed for fewer than 15% of osteoporotic fracture patients11). Another report indicated that osteoporosis treatment is initiated for 1% to 22% of patients with hip fracture 191213). The reason for these low rates is not clear, but physicians, especially orthopedic surgeons, may still be more focused on fracture operation rather than postoperative (PO) treatment. Given the high lifetime risk of osteoporotic fracture1415), evaluation and treatment rates seem to be lower than expected.
Dual-energy X-ray absorptiometry (DXA) and quantitative computed tomography (QCT) are the most common diagnostic modalities for osteoporosis16). QCT can be used to measure BMD in three dimensions and allows to measure volumetric trabecular bone density accurately without superimposition of cortical bone or other tissues. The advantage of DXA is its ability to detect small changes in bone mineral content with low-dose radiation exposure171819), whereas the advantage of QCT is that data on the mineral contents of the cortical and trabecular bones are displayed separately, with the localization of the fracture to be studied. Likewise, QCT and DXA are useful in the diagnosis of BMD with different mechanisms. The superiority of either modality over the other may differ depending on accessibility, patient's pain and gait ability, and other factors. Patients with hip fractures usually need CT scans for evaluation of the fracture pattern and for operative planning. We assumed that if osteoporosis evaluation can be performed along with routine CT for fracture evaluation, this would be better and more effective for osteoporosis treatment after surgery.
Accordingly, our study aimed to evaluate the efficacy of simultaneous CT and QCT in patients with OHF by analyzing the prescription rate of osteoporosis medication in comparison with that of conventional DXA. We hypothesized that simultaneous CT and QCT would increase the prescription rate of osteoporosis medication, as QCT can be performed concurrently with CT without additional movement and tests.
MATERIALS AND METHODS
This prospective study was approved by the Institutional Review Board at Yonsei University College of Medicine (no. 1-2015-0034), and all of the patients provided informed consent.
1. Patients and Settings
This study included consecutive patients older than 65 years who underwent internal fixation or hip arthroplasty for OHF (peritrochanteric or femur neck fracture) between February and May 2015 (Fig. 1). Patients with a medical history of cancerous conditions, rheumatoid disease, or severe comorbidities such as liver or kidney disease were excluded. Patients who had been taking osteoporosis medications were also excluded. We included 108 patients, of whom 6 were lost at follow-up, 3 died from cardiopulmonary disease, and 1 was transferred to another department (Rehabilitation Medicine) in order to receive treatment for osteoporosis; these 10 patients were excluded from the analyses. Finally, 98 patients were included in the study and were assigned to either the QCT or DXA group. The QCT group (47 patients) underwent QCT just after undergoing CT upon admission to the emergency department. The DXA group (51 patients) underwent DXA after surgery, before discharge, or in the outpatient clinic if evaluation was not performed during the admission period. The patients were not randomly assigned. Simultaneous QCT and CT scans were only possible from 6:00 p.m. to 11:00 p.m. on weekdays and from 9:00 a.m. to 6:00 p.m. on weekends in our hospital. Patients who could undergo QCT and CT simultaneously before surgery were assigned to the QCT group. Those who could not undergo QCT and CT simultaneously or who had previously undergone CT in other facilities were assigned to the DXA group.
In the QCT group, all the patients were scanned by using a Somatom Sensation 16 CT scanner (Siemens, Erlangen, Germany) just after hip CT scan. QCT was performed by using the QCT Pro calibration phantom and software system with the CTXA Hip analysis module (Mindways Software, Inc., Austin, TX, USA). In the DXA group, all the patients were scanned by using a Discovery DXA system (Hologic, Inc., Bedford, MA, USA). Closed reduction and internal fixation with the Zimmer Natural Nail System (Zimmer, Warsaw, IN, USA) or Proximal Femoral Nail (DePuy Synthes, Zuchwil, Switzerland) was performed for peritrochanteric fractures, bipolar hemiarthroplasty was performed with a Summit stem and Self-centering System (DePuy Synthes, Warsaw, IN, USA) for displaced femur neck fractures, and multiple screw fixation was performed for non-displaced femur neck fractures. No statistically significant differences in fracture type or operation methods were observed between the two groups (P=0.647). The patients were encouraged to engage in tolerable ambulation exercise using a walker or crutches or range of motion exercise.
No significant difference in the mean length of hospital stay (4.2±2.4 vs. 4.0±1.9, P=0.457) was observed between the two groups. Most of the patients were transferred to other facilities for rehabilitation after discharge (43 patients [91.5%] in the QCT group vs. 45 patients [88.2%] in the DXA group, P=0.426). Outpatient clinic visits after discharge were at PO week 2 for stitch out, and at PO weeks 6 and 12. In both groups, we prescribed osteoporosis medication (bisphosphonate or selective estrogen receptor modulators) according to QCT or DXA results. For the QCT group, because we had already obtained the QCT results for all of the patients before surgery, we prescribed osteoporosis medication before discharge. If osteoporosis medication was not prescribed upon discharge, we prescribed it at every visit to the outpatient clinic. For the DXA group, our routine protocol was to prescribe DXA at PO day 2, but if DXA was not prescribed at that time, it was prescribed at PO week 2 (the first visit to the outpatient clinic) and PO week 6 just before visiting the outpatient clinic. If DXA was not prescribed at PO weeks 2 and 6, it was prescribed at PO month 3. We prescribed osteoporosis medications according to DXA results.
2. Statistical Analysis
The osteoporosis evaluation rate and prescription rate were determined at discharge, and at PO day 2, PO day 6, and PO week 12 during outpatient clinic visits. The results were compared between the groups by using the Student t-test for continuous data and the chi-square test for categorical data. Statistical analysis was performed by using the IBM SPSS Statistics version 20.0 software for Windows (IBM Corp., Armonk, NY, USA). P-values less than 0.05 were considered statistically significant.
RESULTS
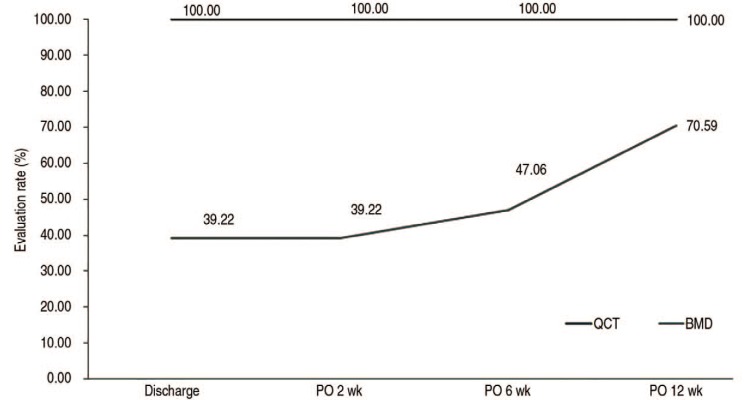
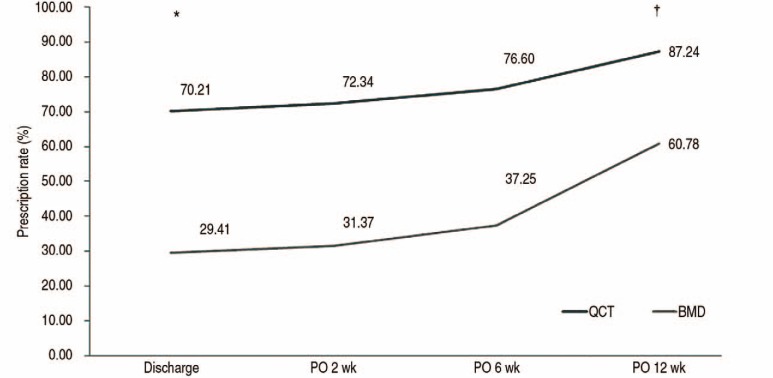
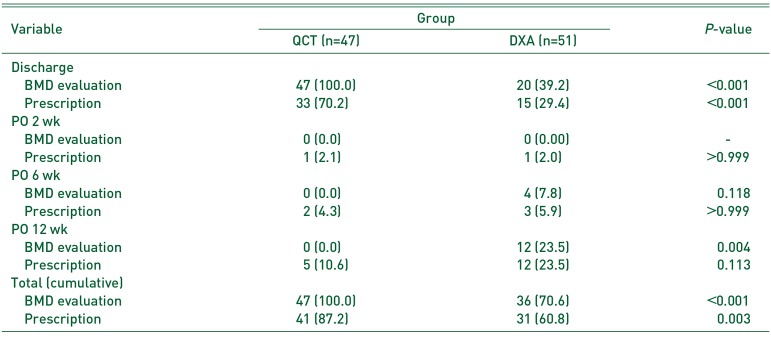
No difference in age was observed between the two groups (Table 1). The mean trabecular BMD of L1-L4 as measured by using QCT was 72.95±4.78 mg/cm3, and the mean BMD of L1-L4 as measured by using DXA was −4.33±0.89. The mean trabecular BMD of the hip as measured by QCT was 73.35±4.9 mg/cm3, and the mean BMD of the hip as measured by DXA was −4.31±0.99 (Table 1). Osteoporosis evaluation rates and physician prescription rates after surgery are shown in Table 2, and Fig. 2 and 3. The osteoporosis evaluation rate by QCT was 100% (Table 2 and Fig. 2) because all of the patients assigned to the QCT group underwent QCT along with hip CT. The osteoporosis evaluation rate by DXA increased from 39.2% at discharge to 70.6% at PO week 12 after surgery (Fig. 2). The difference between the cumulative evaluation rates at the final follow-up at PO week 12 was significant (100% vs. 70.6%, P<0.001; Fig. 2). The difference between the rates of osteoporosis medication prescription at discharge was also significant (70.2% in the QCT group vs. 29.4% in the DXA group, P<0.001), whereas no significant difference was observed at later time points (Fig. 3). A significant difference in cumulative prescription rate at PO week 12 was observed (87.2% in the QCT group vs. 60.8% in the DXA group, P=0.003; Fig. 3).
DISCUSSION
The present study evaluated the efficacy of simultaneous CT and QCT in patients with OHF by analyzing the prescription rate of osteoporosis medications in comparison with that of the conventional DXA. The results demonstrate that simultaneous CT and QCT resulted in a better prescription rate of osteoporosis medications, consistent with our hypothesis.
We should note the limitations of this study. First, although prospectively conducted, this is not a randomized controlled study. We assigned patients to the QCT group when simultaneous performance of QCT and hip CT was possible; otherwise, the patients were assigned to the DXA group. Thus, we assigned the patients according to the possibility of examination before surgery. This non-random assignment may have introduced a bias, even though no significant difference in demographic characteristics was observed between the two consecutive patient groups. To minimize the influence of prescription, the residents who prescribed osteoporosis medication before discharge were blinded to the purpose or concept of the study. However, they were hardly blinded to the method of the study because osteoporosis evaluation was performed during the study period. For this reason, the prescription rates of osteoporosis medication in our study might have been much higher in both groups than other studies2021). However, we believe that if the new evaluation method can increase the prescription rate of antiosteoporosis medication, it would be useful for patients. Second, the radiation dose is well known to be higher in QCT (0.060–3.000µSv) than in DXA (0.009–0.013µSv)22232425). However, the radiation dose in QCT is still within the acceptable range, and performing osteoporosis evaluation is very convenient for patients. Thus, surgeons may consider our new method depending on the situation. The evaluation time was 15.2±2.3 minutes for QCT, whereas for DXA it took an additional 40.0±2.3 minutes to transfer patients from the admission room to the DXA evaluation room and back to the admission room (data not shown). Furthermore, even though DXA evaluation was performed after surgery, the patients complained of severe pain throughout the entire DXA evaluation. Again, surgeons may consider simultaneous QCT and hip CT scans, considering the convenience of evaluation and higher prescription rate of osteoporosis medication. Although the cost may differ among countries, but a QCT test is about 20% cheaper than the BMD test using conventional DXA in our country, indicating that our new method is also less costly.
Patients with OHF have quite high mean mortality rate (15–25% within 1 year of injury) due to accompanying complications and other causes37262728). Moreover, OHFs have a negative impact on patient quality of life over a long period29). According to a study by Boonen et al.30), postinjury quality of life deteriorates in comparison with preinjury quality of life, despite functional recovery. Effective management after OHF treatment is well known to be important for lowering the risk of associated fractures, mortality, and morbidity234). However, it is quite surprising that the rates of evaluation (<15% of the patients11)) and osteoporosis medication prescription (<25% of the patients9101213)) by physicians after OHF are quite low. Surgeons need to care more about osteoporosis treatment after OHF because they are responsible for preventing associated fractures and reducing mortality and morbidity rates. We designed this study because osteoporosis evaluation is often omitted since patients feel severe pain even after surgery. When patients visit the outpatient clinic later, orthopedic surgeons often seem to neglect to evaluate them for osteoporosis because they tend to focus on the treatment of the fracture itself. We believe that evaluating osteoporosis simultaneously with routine OHF evaluation on hip CT would be helpful for prescribing osteoporosis medication after surgery. As we hypothesized, physician prescription rate significantly improved until PO month 3 when QCT was performed simultaneously with hip CT. We hope that our new method would help surgeons improve the management of osteoporosis and also be convenient for patients.
Some studies have suggested that bisphosphonate appears to delay fracture healing3132), whereas other studies reported that early initiation of bisphosphonate does not affect healing or clinical outcomes of osteoporotic fractures3334). Despite this controversy, we prescribed bisphosphonate after fracture surgery, because we thought that minimizing the number of patients with missed opportunity of osteoporosis treatment after hip surgery would be more beneficial than the potential negative effect of bisphosphonate on fracture healing.
CONCLUSION
Our new method of simultaneous CT and QCT significantly increased the osteoporosis evaluation and prescription rates in patients with OHF. The use of this method may enable appropriate and consistent prescription of osteoporosis medications, eventually leading to patient medication compliance. Moreover, we expect this simultaneous scanning to contribute to the reduction of subsequent fractures, mortality, and morbidity through PO care for osteoporosis in patients with OHF.


 XML Download
XML Download