

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Septic arthritis of the hip is more frequent in the pediatric population than the adult population. Early diagnosis and prompt intervention to preserve normal structure and recover full joint function is mandatory in children with acute septic arthritis of the hip since the result can be an unfavorable outcome and life-long disability1,2). The surgical options include repeated aspirations, open arthrotomy, and arthroscopic drainage3,4). Recently, several reports described successful outcomes in children following arthroscopic management of septic hips5-7). The immature anatomical features and smaller hip joints of young children make arthroscopic procedure technically challenging8), and require specialized instruments, such as smaller arthroscopes and a fracture table for traction. However, little information is available concerning arthroscopic surgical techniques for children. We report the case of the arthroscopic management of acute septic arthritis of the hip joint in 3-year-old child using a 30°, 2.7 mm arthroscope for the ankle joint on the general table. Her parents were informed that data concerning her case would be submitted for publication.
Case Report
A 3-year-old female child was complaint of fever, limping gait, and right groin pain in the emergency room. As a past medical history, she had an upper respiratory infection, which had completely resolved two weeks ago. There were no abnormal symptoms in patient until the day before her presentation to the emergency room.
In the emergency room, the body temperature was checked 38℃ with normal pulse rate and blood pressure. On physical examination, right hip joint motion was limited by pain and warmness of the anterior aspect of the right groin was detected. However, there was no tenderness or redness on the right hip joint. A simple radiograph of the pelvis did not reveal destructive joint lesions, except for a mild soft tissue swelling of the hip joint. An magnetic resonance imaging (MRI) scan could not perform due to patient's noncooperation. Hematological examination revealed a leukocyte count (WBC) of 15,440/ml (normal range, 3,000-9,000/ml), a C-reactive protein (CRP) of 42 ng/ml (normal range, 0-5 ng/ml) and a erythrocyte sedimentation rate (ESR) of 60 mm/hr (normal range, 0-20 mm/hr). Analysis of fluid aspirated from the affected joint revealed a leukocyte count of 54,000/ml with 99% neutrophils, confirming acute septic arthritis of the hip joint4,9).
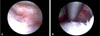
The patient was placed in a supine position on a general table. Under general anesthesia, two arthroscopic portals (anterolateral and ancillary portals) of the hip were used (Fig. 1A). We initially approached the peripheral compartment via the anterolateral portal as a viewing portal using a 30°, 2.7-mm arthroscope for the ankle joint, which was made 0.5 cm distal and 1 cm anterior to the tip of the greater trochanter. The ancillary portal as a walking portal was placed 2.5 cm distal portion to the anterolateral portal (Fig. 1B). After setting up the two portals, the arthroscope, various instruments, and the motorized shaver were switched between portals. Synovectomy at the femoral neck junction was performed and the central compartment was approached with manual traction. After pelvis was fixed by first assistant, the joint space was distracted about 10 mm by second assistant's manual traction and was maintained during surgery in the central compartment. The hip joint was lavaged by the arthroscope with 10 L of normal saline solution and debrided by the motorized shaver (Fig. 2). Before the portals were closed, a suction drain tube was placed in the peripheral compartment to avoid hampering the drain tube between the femoral head and the acetabulum.
After the arthroscopic drainage, intravenous firstgeneration cephalosporin (cephazolin) was administered empirically. The causative microorganism was not identified in the hip joint culture and intravenous antibiotic was maintained 3 weeks. Tolerable motion of hip joint and weight bearing on the foot was allowed immediately after surgery. The suction drain was removed at 2 days post-operatively. Elevated WBC, CRP and ESR count were normalized postoperative 12 days. The range of motion of right hip joint was recovered at 2 weeks after surgery. There was no recurred signs and radiological changes at the final follow-up at 2 years postoperatively.
Discussion
Hip arthroscopic treatment is considered as an attractive alternative to open arthrotomy in septic arthritis in the pediatric population10). The surgical technique of hip arthrocopy in children is similar to that performed in adults, but multifarious anatomical and pathoanatomical characteristics, such as a smaller joint space, lager neck-shaft angle, femoral anteversion and the presence of the physis, make hip arthroscopy in children technically challenging8). There have been several reports of successful outcomes in pediatric patients following arthroscopic management of septic hips5,6), however little information is available concerning surgical intervention in children and there was no appropriate arthroscopic equipments. This case report shows usefulness of arthroscopic treatment of early stage septic hip arthritis in child and ankle arthroscope could be possible appropriate instrument in these age groups.
Advanced instrumentation is required to overcome the arthroscopic limitations posed by a confined hip joint in pediatric patients. However, previous reports described arthroscopic management of septic hip using a constant size scope and same surgical technique, regardless of pediatric age5,6). This case report indicates the success of arthroscopic treatment using a 2.7 mm arthroscope for the ankle joint without the specialized instruments on the general table for a 3-year-old child.
In the present case, only two portals (anterolateral and ancillary portal) and an arthroscope for the ankle joint were used on the general table. Using the ancillary portal as working portal, synovectomy in the peripheral compartment, such as around the femoral neck junction, was performed and the central compartment was approached with manual traction. Especially, care should be taken that you need to allow sufficient joint space to prevent physis damage when you access to the central compartment. Without using the anterior and posterolateral portals, we were able to sufficiently treat the septic arthritis; this approach could minimize nerve and vessel injury in a child patient. However, in performing an arthroscopy in the smaller hip joint of a child, the surgeon should be aware of the age-related diversity of joint anatomy. Furthermore, a substantial learning curve period should be anticipated for this patient population.
Conclusion
We successfully treated a case of acute septic arthritis in the hip joint of a 3-year-old child using a 2.7 mm arthroscope for the ankle joint through manual traction without a traction table. This procedure might be more helpful in minimizing scarring and damage of hip anatomy, and facilitating earlier rehabilitation.

 XML Download
XML Download