

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Compliance with treatment is one of the fundamental factors of effective cancer management. Most malignancies have high tumor growth rates and risks of metastasis, and non-compliance with treatment (NCT) or delayed treatment can result in disease progression and worsened survival.[12] Non-compliance is sometimes observed because patients seek a second opinion, doubt modern medicine, and use complementary and alternative medicine instead of standard treatment.[34] Furthermore, some patients refuse to get any treatment because of old age, fear of operations or misunderstandings of standard treatment.
In Korea, newly diagnosed cancer-related information has been collected by the Korea Central Cancer Registry (KCCR) since 1999. This information includes patient demographics and tumor characteristics including age, sex, region, primary cancer site, histological type, and the Surveillance, Epidemiology, and End Results (SEER) stage. Moreover, data regarding whether any treatment was applied within 4 months of diagnosis are also collected. Most patients received some treatment within 4 months; however, some patients delayed treatment or never receive any treatment.
In this study, we defined patients who did not receive any treatment within 4 months after diagnosis as patients with NCT, and searched for related annual trends and evaluated the influence of NCT on survival.
MATERIALS AND METHODS
Data sources
The KCCR, a nationwide, hospital-based cancer registry, was launched by the Ministry of Health and Welfare of Korea in 1980. This registry has collected information on cancer from the entire Korean population from more than 150 training hospitals and integrated regional cancer cancers [5]. Annually, the KCCR provides nationwide cancer incidence, survival, and prevalence statistics.
The KCCR obtained information about newly developed gastric cancer cases between 1999 and 2014 with the codes C16.0–16.9 according to the tenth revision of the International Statistical Classification of Disease and Related Health Problems (ICD-10) [6]. The KCCR records include the best available information on the treatments for gastric cancer and the stages at diagnosis as they appear in the medical records within 4 months of diagnosis. Treatment was divided into three categories in this study: surgery only, surgery with chemotherapy, chemotherapy only, and other. Stage at diagnosis was reported based on the SEER system and classified as localized (invasive cancer confined to the organ of origin), regional (spread to adjacent organs and/or regional lymph nodes by direct extension), distant (extension to organs other than those covered in the regional category or metastases to distant organs or distant lymph nodes), or unknown. Because data regarding the stage at diagnosis have been formally collected since 2006, the analysis of stage at diagnosis was performed for the years between 2006 and 2015.
In the survival analysis, we evaluated relative survival rates using demographic data from the KCCR and mortality data from Statistics Korea [7]. Relative survival rate is the ratio of the observed survival rate among gastric cancer patients to the expected survival rate among age- and sex-matched individuals from the general population. As patients may die of various causes, gastric cancer-specific survival rate can be assumed by comparing the expected survival rate of the general population. A relative survival rate of 100% indicates that the patient's survival rate is the same as that of the age- and sex-matched general population.
Statistical analysis
The age-standardized incidence rates per 100,000 people were calculated by dividing the sum of the expected age-specific rates by the sum of the standard population [8]. The sum of the expected age-specific rates was obtained by multiplying the age-specific incidence rates among the study population by the proportion of the population in the corresponding age-specific group among the standard population. We used Segi’s world population as the standard population [9].
The relative survival rates were calculated using the Ederer II method based on an algorithm written in SAS by Dickman with some minor adaptations [1011]. Asymmetric observed survival confidence intervals (CIs) were formed from standard errors that were estimated using Greenwood's method and a log (-log) transformation [12]. The confidence limits of the relative survival rate were derived by dividing the observed survival limits by the corresponding expected survival rate. The median survival rate using the Kaplan-Meier method and its confidence intervals were calculated, and the statistical significances of the differences between the 5-year relative survival rates were defined if the 95% CIs did not overlap between the 5-year survival rates. All analyses were conducted using SAS 9.3 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
This study was approved by the Institutional Review Board of the National Cancer Center (NCC2017-0012) and was performed in accordance with the principles of the Declaration of Helsinki. The need for informed consent was waived on account of the retrospective nature of the study, and because the data were de-identified prior to analysis. The authorization for data processing was obtained from the National Cancer Act.
RESULTS
Overall trend of NCT for gastric cancer in the recent 16 years
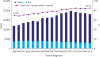
The proportion of NCT gradually decreased from 30.6% (5,870/19,158) in 1999 to 15.3% (4,434/24,589) in 2015 (absolute difference [AD], −15.4%; 95% CI, −16.1, −14.6; P=0.004; Fig. 1, Supplementary Table 1).
Changes in patterns of treatment of gastric cancer
The proportion of patients who underwent surgery (including endoscopic treatment) for gastric cancer increased from 61.0% in 1999 to 77.7% in 2015 (AD, 16.7%; 95% CI, 15.7, 17.7; P=0.005; Table 1). The proportion of patients who underwent surgery with chemotherapy gradually decreased from 27.4% in 1999 to 13.9% in 2015 (AD, −13.5%; 95% CI, −14.4, −12.6; P=0.004). In contrast, patients received chemotherapy in similar proportions ranging from 7.4% to 10.1% during the same period.
Table 1
Patterns of treatment for gastric cancer
Trend of NCT according to the age and SEER stage, from 2006 through 2015
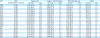
Table 2 presents the NCT according to the age group and SEER stage and its changes between 2006 and 2015. The proportion of NCT increased with increasing age, from 9.2% in patients younger than 40 years to 72.9% in those older than 80 years in 2006, and a similar pattern of change from 5.4% to 55.0% was observed in 2015. Regarding changes in the NCT between 2006 and 2015, the proportions of NCT decreased in all age groups (AD, −3.8, −4.1, −5.7, −10.0, −18.8, and −17.9 for the ascending age groups).
Table 2
NCT according to the age group and SEER stage between 2006* and 2015
The proportions of NCT also increased according to the SEER stage. In 2006, the NCT rates were 17.6% among those with localized disease and 35.5% among those with distant metastasis, and a similar pattern was observed in 2015. In terms of the changes in NCT between 2006 and 2015, the rate also decreased in all SEER stages (AD, −8.2, −2.0, and −2.8 for the local, regional, and distant stages, respectively).
Overall incidence of NCT according to age group and SEER stage, from 2006 through 2015
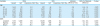
From 2006 through 2015, the overall incidence rates of NCT were analyzed according to the age groups and SEER stages (Table 3). In localized disease, the proportions of NCT were 4.3% in the age group below 40 years, and 46.8% in the age group of 80 years or more. In distant metastasis, the proportions were 12.2% in the age group below 40 years and 77.1% in the age group of 80 years or more.
Table 3
NCT according to the age group and SEER stage during the 2006*–2015 periods

Survival rates according to the SEER stage by time
The relative survival rates between patients who were diagnosed with gastric cancer in the period of 2006–2010 and 2011–2015 in each SEER stage are presented in Fig. 2 (Supplementary Table 2). When we compared the 5-year relative survival rates between the patients who were treated within 4 months and those with NCT during 2006–2010, the NCT group had significantly lower survival rates overall and in each SEER stage (77.0% (95% CI, 76.8, 77.3) vs. 31.2% (95% CI, 30.6, 31.8) in overall, 99.2% (95% CI, 99.0, 99.3) vs. 57.6% (95% CI, 56.4, 58.8) in the localized, 62.4% (95% CI, 61.8, 63.1) vs. 12.4% (95% CI, 11.3, 13.5) in the regional, and 8.4% (95% CI, 7.9, 9.0) vs. 3.0% (95% CI, 2.6, 3.5) in distant stages, respectively).
Fig. 2
Relative survival rates between patients who were diagnosed with gastric cancer in 2006–2010 and 2011–2015 according to each SEER stage: (A) overall; (B) localized; (C) regional; (D) distant.
NCT = non-compliance to the treatment; SEER = surveillance, epidemiology, and end results.

When we compared the 5-year relative survival rates between the 2006–2009 and 2010–2015 periods, slight increases in the 5-year relative survival rates were observed overall and in the localized, and regional stages among the treated patients (from 77.0% to 83.1%, from 99.2% to 99.7%, and from 62.4% to 67.1% in overall, localized, and regional stages, respectively). However, the 5-year relative survival rate exhibited no significant difference in the distant stage between the 2006–2009 and 2010–2015 periods (8.4% vs. 8.3%). In the NCT group, there were no significant differences in the 5-year relative survival rates overall or in any of the SEER stages between 2006–2009 and 2010–2015.
DISCUSSION
In this study, we searched for trends in NCT among gastric cancer patients; NCT was defined by the lack of receipt of any treatment within the 4 months after diagnosis according to the national cancer registry database. The overall incidence of NCT continuously decreased from 1999 to 2015, but the NCT rate is still currently 15.3% among gastric cancer patients. The proportions of NCT were higher in the old age group and among those in the distant stage, and it decreased in all age groups and stage subgroups between 2006 and 2015. The relative survival rates according to SEER stage were definitely lower in the NCT group than in the treated group.
NCT, as defined in this study, includes both patients who simply delayed treatment and those who did not receive any treatment throughout their lives (untreated patients). Regarding simple treatment delay, some studies have reported detrimental effects on survival in cancers of the breast, lung, rectum, and head and neck, and prompt treatment initiation for cancer has been emphasized [121314]. In contrast, other studies have found no significant effect of treatment delay on survival in cancers of the bronchus, pancreatic head, cervix, prostate, and colon [315161718]. Therefore, reasonable delays, such as those committed for ovarian preservation, an exact diagnosis, and transition to a qualified hospital, are considered acceptable.
Regarding those who receive no treatment for cancer, few studies have reported on the prognoses of untreated patients thus far [192021]. In previous studies, the medical charts of untreated patients have been reviewed in large-volume centers, and an analysis using the national cancer database was recently conducted. The prognoses of the untreated patients were obviously poorer than those of the treated patients in these studies. For gastric cancer, only a few studies have reported on the natural history of early gastric cancer, and the time from early gastric cancer to advanced gastric cancer or death has been the focus of these previous studies [2122].
Although we could not differentiate the two types of patients due to limitations in our data, we suggest that a considerable number of NCT patients could be patients who did not receive any treatment in all their lives (untreated patients). In Korea, the National Health Insurance has covered the entire nation since 1989, and most cancer patients can visit and receive optimal treatment in specialized high-volume centers within several weeks [23]. Therefore, a patient failing to receive treatment within 4 months after the diagnosis of cancer is highly suggestive of his rejection of standard treatment in Korea. Moreover, the definite difference in relative survival rates between the treated and NCT patients also supports the notion that a considerable number of NCT patients could be untreated.
The predictive factors of non-compliance have been evaluated in several studies. Old age, lack of insurance, low income, severe comorbidity, and advanced cancer stage were associated with receiving no treatment [2425]. However, we observed that approximately 5% of young patients with localized cancer were NCT, and possibly rejected treatment for treatable gastric cancer. Personal distrust of medical treatment and misunderstandings of cancer could have affected these patients' decisions. Complementary and alternative medicine use could also influence treatment delays because Korean culture has a long history of traditional medicine [26].
The high proportion of NCT patients among old patients is also noticeable in this study. More than 15% of the septuagenarian and more than 40% of the octogenarian patients were NCT even though they had localized gastric cancer. Korea is rapidly becoming an aging society and is expected to achieve the highest life expectancy in the world [27]. Septuagenarians are very common patients with gastric cancer in routine clinical settings, and the frequency of octogenarian patients is also increasing in Korea. Considering the favorable outcomes of elderly patients who are treated for gastric cancer, we need to care for these patients more actively so that more elderly patients receive the correct treatment [28].
Recently, the national cancer statistics of Korea showed a rapid increase in survival rates and a decrease in mortality rates of gastric cancer patients [7]. Early detection due to the generalization of the National Cancer Control program is considered to be a critical factor for good prognosis [29]. In this study, we found that the proportion of NCT has continuously decreased with time and suggested that decreased NCT could also influence favorable survival outcomes. However, NCT patients still considerably existed, and further efforts and national strategy to reduce the NCT patients are necessary.
This study has several limitations. First, as we described previously, the NCT patients included both patients who only delayed treatment and those who did not receive any treatment for cancer. Because the KCCR contains treatment information for the 4 months after diagnosis, we could not define final treatment statuses in this study. Second, NCT was evaluated only according to the age and SEER stage. However, many factors, such as private health insurance, socioeconomic status, and comorbidity, have been analyzed in other studies, but we focused on age and SEER stage as the most important clinical factors. Nevertheless, we believe that the KCCR data, which contains information that is over 97% complete and encompasses the entire South Korean population, might allow for analyses with high internal validity and generalizability [7]. Finally, the SEER staging system differs from the tumor-node-metastasis staging system, which is commonly used in the clinical setting. The localized SEER stage includes stage I and II cancers according to the TNM staging system, and the regional SEER stage includes stage I–III cancers. Therefore, clinicians should consider this different staging system in interpreting the results of this study.
In conclusion, the proportion of NCT gastric cancer patients has decreased during the last 16 years. However, a considerable proportion of elderly patients were still NCT, and NCT was observed even among young patients with localized disease. There must be a strategy to decrease NCT and improve the nationwide survival rate of patients with gastric cancer.
 XML Download
XML Download