

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Laparoscopic surgery for gastric cancer has been widely practiced since it was first described in 1994 [1]. However, there are insufficient multi-institutional prospective randomized controlled trials (RCTs) comparing the surgical safety and long-term outcomes of laparoscopic distal gastrectomy (LDG) with those of open distal gastrectomy (ODG). Multicenter prospective RCTs, such as the KLASS-01 study in Korea [2] and JCOG 0912 study in Japan [3], showed favorable short-term outcomes for LDG in early gastric cancer (EGC), with lower postoperative wound complication rates, less intraoperative bleeding, and shorter hospital stays, but long-term outcomes have not been reported. The CLASS-01 study in China [4] is the only multicenter study of surgical safety in advanced gastric cancer (AGC) and showed comparable postoperative morbidity for LDG and ODG. The JLSSG 0901 study in Japan [5] demonstrated the technical safety of LDG for AGC in a phase II trial and is on-going to confirm the non-inferiority of LDG to ODG in terms of long-term outcomes. Some meta-analyses and 1 case-matched study showed short-term benefits including reduced wound complication rates for laparoscopic gastrectomy (LG) in AGC [6789]. However, 2 RCTs reported similar rates of postoperative complications for LG and open gastrectomy (OG) [410] and 1 RCT demonstrated that anastomotic leakage tended to be more frequent in LDG than in ODG [4]. Therefore, the short-term benefits of LG remain unclear. Although many retrospective cohort studies have compared the long-term outcomes of laparoscopic surgery with those of open surgery in AGC [11121314], to the best of our knowledge, only 1 small RCT [10] reported these data. This RCT demonstrated that laparoscopic gastrectomy in AGC is a safe and feasible procedure with good curability and survival rates comparable to those of open surgery. Although a few meta-analyses [67915] and case-matched studies [16171819] concluded that the long-term results of open and laparoscopic surgery were comparable, some studies included in the meta-analyses compared unmatched groups of patients [79]. Therefore, definitive evidence for survival is needed.
This study was designed to evaluate short-term and long-term outcomes in patients who underwent LDG compared with those of well-matched patients who underwent ODG for gastric cancer to acquire further evidence supporting this widely-performed procedure.
MATERIALS AND METHODS
This study investigated 384 patients who were diagnosed with pathologic stage II and III gastric cancer after distal gastrectomy from July 2006 to November 2016. All patients were given sufficient information and written informed consent was obtained. This study was approved by the institutional review board of Kyung Hee University Hospital at Gangdong. Among the 384 patients, the following were excluded: 33 with follow-up loss after surgery, 25 with clinical T1N0 stage, 23 whose medical records did not provide an accurate clinical stage, 5 who underwent emergency surgery due to cancer perforation, 3 with a history of gastric surgery, 2 with double primary cancer (colon cancer, hepatocellular carcinoma), 2 who had undergone endoscopic submucosal dissection, 1 with remnant gastric cancer, 1 who received concomitant nephrectomy, and 1 with para-aortic lymph node metastasis on clinical staging. The remaining 288 patients were recruited to our study and were divided into 2 groups according to the operative method (open versus laparoscopic). We performed propensity score matching analysis to minimize bias between the LDG group and ODG group. Propensity scores were calculated using a logistic regression model and the following variables: sex, age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, clinical tumor staging (cTNM), pathological tumor staging (pTNM) according to the American Joint Committee on Cancer/Union for International Cancer Control 7th edition, histologic grade, tumor size, and adjuvant chemotherapy. After 1:1 propensity score matching, 60 patients were included in the LDG group and 60 in the ODG group.
The following variables were obtained from our prospective gastric cancer database: patient and tumor characteristics; surgical outcomes including the length of resection margin, extent of lymph node dissection, number of retrieved lymph nodes, and operative time; and postoperative outcomes including recovery, complications, and mortality. Postoperative complications and mortality were defined as those occurring within 30 days after surgery. Postoperative complications were considered either surgical or medical and either Grade I/II or Grade III/IV using the Clavien-Dindo Classification (CDC) [20]. Tumors were pathologically classified in accordance with the Japanese Classification of Gastric Carcinoma, 4th English edition [21]. Papillary or tubular adenocarcinomas were classified as differentiated adenocarcinomas, and poorly differentiated, signet-ring cell, or mucinous adenocarcinomas as undifferentiated adenocarcinomas, in accordance with the histological classification of the World Health Organization. All procedures were performed by 3 surgeons with experience of more than 100 gastric surgeries. We tried to perform D2 lymph node dissection in patients who were diagnosed with AGC preoperatively according to the treatment guidelines of the Japanese Gastric Cancer Association, and the extent of lymphadenectomy was decided by the operative record and not by the pathology report. Clinical stage was decided by the combination of preoperative endoscopic findings, stomach or abdominopelvic computed tomography, and/or positron emission tomography-computed tomography. The LDG and ODG groups were compared for the following short-term outcomes after gastrectomy: operative time, number of retrieved lymph nodes, time to resumption of food intake, postoperative hospital stay, and postoperative complications. To assess long-term outcomes, recurrence-free and overall survival rates were evaluated and compared between the LDG and ODG groups.
Statistical analysis
Categorical data were compared with the χ2 test or Fisher's exact test, as appropriate. The Mann-Whitney test was used to compare continuous variables. The length of recurrence-free survival (RFS) and overall survival (OS) was assessed. Survival curves were plotted using the Kaplan-Meier method and compared with the log-rank test. A P-value <0.05 was considered significant. All statistical analysis was performed with R version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/).
RESULTS
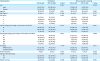
The clinicopathological characteristics of the unmatched and matched patient populations are summarized in Table 1. Before propensity score matching, there seemed to be significant differences in BMI (P=0.096), ASA score (P=0.083), cTNM (p<0.001), tumor size (P=0.001), and use of adjuvant chemotherapy (P=0.087) between the LDG and ODG groups. However, there was no significant difference between the 2 groups after propensity score matching. Because of poor general condition, refusal of further treatment by the patient or family, or advanced age, some AGC patients did not receive adjuvant chemotherapy.
Table 1
Clinicopathological characteristics
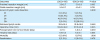
Perioperative outcomes are shown in Table 2. The extent of lymph node dissection in the LDG group (D2/D2+, 76.7%) was more limited than in the ODG group (D2/D2+, 91.7%) (P=0.002); however, there was no difference in the number of retrieved lymph nodes between the 2 groups (LDG vs. ODG, 30.5±15.5 vs. 32.8±16.9). Operative time was significantly longer in the LDG group (234.8±46.9 minutes) than in the ODG group (217.2±48.0 minutes) (P=0.045), whereas time to resumption of food intake (4.7±1.1 days vs. 5.6±3.3 days, P=0.049) and length of hospital stay (9.6±4.3 days vs. 11.5±5.1 days, P=0.035) were shorter in the LDG group than in the ODG group. Mortality and readmission rates were similar between the 2 groups.
Table 2
Perioperative outcomes
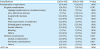
Postoperative complications are summarized in Table 3. The incidence of all-grade overall, surgical, and medical complications did not differ significantly between the LDG and ODG groups (13.3% vs. 13.3%, P=1.000; 8.3% vs. 11.7%, P=0.761; and 6.7% vs. 3.3%, P=0.675; respectively). Severe overall complications ≥CDC IIIa were similar in the 2 groups (LDG vs. ODG, 6.7% vs. 5.0%, P=1.000). Individual surgical complications, cardiac complications, and pulmonary complications also did not differ significantly between the groups.
Table 3
Postoperative complications
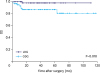
The median overall follow-up period was 38.5±26.8 months, with 38.5±22.8 months in the LDG group and 38.5±30.8 months in the ODG group. The Kaplan-Meier survival curves after propensity score matching are shown in Figs. 1 and 2. Before matching, 3-year RFS did not differ significantly between the LDG and ODG groups (86.3% vs. 78.7%, P=0.35); however, 3-year OS was significantly longer in the LDG group than in the ODG group (98.0% vs. 85.7%, P=0.0121). After matching, 3-year RFS did not differ between the LDG and ODG groups (86.3% vs. 75.3%, P=0.259); however, 3-year OS was longer in the LDG group (98.0% vs. 86.9%, P=0.0176). In subgroup analysis, 3-year RFS and 3-year OS did not differ significantly between the LDG group and ODG group for stage II disease (3-year RFS, 91.0% vs. 90.7%, P=0.632; 3-year OS, 100.0% vs. 91.9%, P=0.068) or stage III disease (76.8% vs. 45.2%, P=0.0827; 94.1% vs. 76.1%, P=0.104, respectively).

DISCUSSION
The results of this study suggest that LDG might be a promising treatment for clinical and pathological AGC in terms of short-term and long-term outcomes. One small RCT and a few retrospective case-matched studies on AGC showed no significant differences in overall survival between LG and OG [1016171819]. Similar survival was also reported in retrospective cohort studies of patients with AGC who underwent gastrectomy [11121314]. Our results are consistent with the findings of previous studies. However, the present study included only patients with clinical and pathological diagnoses of AGC as well as well-matched variables. In our study population, the 3-year OS rate in the LDG group was higher than in the ODG group, probably because the LDG group tended to have lower clinical and pathological staging than the ODG group, although the difference was not statistically significant. Moreover, the small number of patients in the study and the insufficient follow-up period made it difficult to determine long-term survival rates. The ultimate explanation can be derived from previous colon cancer research [22], which demonstrated that stage III patients who underwent laparoscopic colectomy had a higher survival rate than patients with open colectomy, and proposed that this was due to the impact of laparoscopy on the surgical stress response, cellular immunity, cytokine release, intraoperative tumor manipulation, complication rates, and blood transfusion factors. In a western study comparing LG with OG, the OS and RFS did not differ significantly, although the follow-up period was not equal between the 2 groups and some early-stage cancers were included [23].
In this study, the extent of lymphadenectomy was significantly limited in the laparoscopic group compared to the open group. According to the Japanese Gastric Cancer Treatment Guidelines [21], D2 lymph node dissection is the standard treatment for curable cT2-T4or cT1N+ gastric cancer; however, 23.3% of the LDG group and 8.3% of the ODG group underwent lymphadenectomy that was less than D2. Although not shown in the results, limited lymph node dissection was reported in 31.8% (7/22 patients) of the LDG group and in 11.8% (2/17) of the ODG group among cTNM IB patients, and 24.1% (7/29) and 9.1% (3/33), respectively, among cTNM II patients. All cTNM III patients received standard D2 lymph node dissection. Despite the high rate of limited lymphadenectomy in the laparoscopic group, there was no difference in survival between the 2 groups. This result suggests that the standard treatment of D2 lymphadenectomy may not be necessary in patients with clinical T1b or TII disease, consistent with previous reports [242526]. Moreover, the therapeutic index for No. 11p and 12a dissection in earlier advanced disease was decreased in the COACT1001 study [27]. An ongoing multi-institutional RCT [28] is expected to clarify the optimal extent of lymph node dissection for patients with cTNM IB/II gastric cancer.
Our study showed earlier resumption of oral intake and earlier discharge with LDG than with ODG; these results are supported by the findings of previous studies on AGC [791016], and are mainly due to changes in postoperative patient care, especially the dietary schedule. Since 2010, a number of studies have confirmed the safety and efficacy of the Early Recovery after Surgery (ERAS) program in gastric cancer [2930313233]. In our hospital, the dietary schedule was accelerated by 1 day since 2013, although the ERAS program was not applied. During this period, 48.3% (29 of 60 patients) of the LDG group and 25.0% (15/60) of the ODG group were enrolled. Otherwise, the dietary schedule was determined by the recovery of bowel motility and severity of abdominal pain. Although we did not evaluate the postoperative time to first flatus and the visual analog scale or number of injected analgesic doses for pain assessment, our finding of no difference in readmission rates or surgical complications such as postoperative ileus or delayed gastric emptying in both groups indirectly demonstrates the safety of earlier resumption of oral intake in the LDG group.
Postoperative complications did not differ significantly between LDG and ODG groups in our study, concordant with 2 RCTs [410] and 2 propensity score matched analyses [1618]. However, some case-matched studies and meta-analyses showed that the overall complication rates were significantly lower in the laparoscopic group than in the open group [6789]. Regarding specific complications, 1 RCT [10] reported that pulmonary infection was observed more frequently in the open group and 1 case-matched study [8] demonstrated that wound infection was significantly more common in the open group than in the laparoscopic group, whereas our results showed similar rates in both groups. Overall, studies to date suggest that the laparoscopic group shows results that are better or similar to those of the open group, and that laparoscopy may be superior with regard to surgical safety.
Limitations of our study are as follows: we investigated only a small number of patients in a single institution; the follow-up periods were insufficient to obtain longer survival data; and despite good propensity score matching, the slight imbalance in pathologic stage, an important factor that affects survival, could create a hidden bias. We believe that this study could serve as important background research for future RCTs on LDG for AGC.
LDG is safe and feasible in terms of recovery after surgery and long-term oncologic outcomes. LDG may be a treatment option for both AGC and EGC.
 XML Download
XML Download