

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Collision tumors with adenocarcinoma and neuroendocrine elements are commonly diagnosed in the gastrointestinal tract. However, the occurrence of neuroendocrine carcinoma (NEC) in the gastrointestinal tract is rare, ranging from 1% in the esophagus, 0.2% in the colon, and 0.1% to 0.4% in the stomach.1 Herein, we present a case of a mixed adenoneuroendocrine gastric tumor and review the English literature pertaining to such tumors.
Case Report
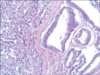
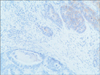
A 77-year-old Caucasian woman was admitted to our department with nausea, anorexia, weight loss, and anemia. The medical history of the patient did not include any significant prior illness. The findings of physical examination were unremarkable. The patient's hemoglobin level (10.3 g/dl) and tumor marker levels (carcinoembryonic antigen, carbohydrate antigen 19.9, and carbohydrate antigen 72-4) were within the normal range. Esophagogastroduodenoscopy revealed a large (>7 cm) ulcerative mass (Borrmann type 3) in the greater curvature of the stomach. Biopsy showed the presence of an adenocarcinoma with moderate differentiation. Computed tomography did not show distant metastasis. The patient underwent D2 subtotal gastrectomy, with no surgical complications. Histopathological analysis showed, in agreement with the diagnosis of a mixed gastric adenoneuroendocrine carcinoma (Fig. 1), that 30% of the tumor area was intensely positive for chromogranin (Fig. 2) and synaptophysin (Fig. 3), with part of it being tubular adenocarcinoma (G2) and of the rest being neuroendocrine large cell carcinoma (G3). The tumor penetrated the serosa, but none of the 29 regional lymph nodes showed metastasis and no distant metastasis was detected (pT4a, pN0, pM0, stage IIb according to the 7th edition of the American Joint Committee on Cancer TNM classification). The lymphatic and vascular lumina were not invaded, but perineural invasion was present. The post-operative course was uneventful. The patient underwent adjuvant chemotherapy, consisting of a combination of cisplatin, doxorubicin, and vincristine, and at the 6-month follow-up, the patient was alive without evidence of recurrence.
Discussion
Collision tumors rarely occur in the gastrointestinal tract. Sporadic cases have been described, with less than 20 cases of such tumors in the stomach being reported, most often from eastern countries. The histological origin of composite tumors is unclear. Neuroendocrine tumors arise from embryonal neural crest cells, which are abundant in the epithelia of the gastrointestinal tract. In fact, some authors have postulated the proliferation of pluripotent precursor cells.2 Lewin and Appleman3 classified gastric cancer into five groups: carcinoma with interspersed neuroendocrine cells, composite glandular-endocrine carcinomas, collision tumors (present case), amphicrine tumors, and a combination of all the above. In 2005, Fujiyoshi et al.4 revised the classification of mixed endocrine and non-endocrine epithelial tumors. This new classification included six groups: neuroendocrine cells interspersed within carcinomas; carcinoids with interspersed non-endocrine cells; composite glandular-neuroendocrine cell carcinomas containing both areas of a carcinoid component and conventional carcinoma; collision tumors in which neuroendocrine tumors and conventional carcinoma are closely juxtaposed, but not admixed (present case); amphicrine tumors predominantly composed of cells exhibiting concurrent neuroendocrine and non-endocrine differentiation; and combinations of the previous types.4 In 2010, the World Health Organization classification of gastrointestinal tumors classified mixed tumors into three groups according to prognosis: high-grade malignant (mixed adenoma/adenocarcinoma-neuroendocrine carcinoma; present case), intermediate-grade malignant (mixed adenocarcinoma G1/G2 neuroendocrine tumor), low-grade malignant (adenoma-neuroendocrine tumor).5
We reviewed the English literature pertaining to gastric mixed tumors (Table 1)6,7,8,9,10,11,12,13,14,15,16,17,18,19,20 and found that most such cases have been reported from eastern countries, probably because of the overall high incidence of gastric tumors in these countries. The 5-year survival rate is lower for these patients than for those with gastric adenocarcinoma. The neuroendocrine component may have a considerable impact on the prognosis.21 Because of the mixed component of the tumor, treatment should focus on parts of the tumor with the more aggressive cells. In cases of well-differentiated neuroendocrine components with benign or low-grade malignant behavior, chemotherapy should focus on the exocrine component. In contrast, in cases of small cell NEC or large cell NEC, the endocrine component should be the main target of the therapy.17
After radical surgical resection, a chemotherapy regimen consisting of cisplatin, doxorubicin, and vincristine is highly recommended.
Mixed adenoneuroendocrine tumors are rare, but they are now well classified. Multimodal treatment should be the aim for these patients because of the neuroendocrine component of the tumor.


 XML Download
XML Download