

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The advent of the flexible endoscope and its world-wide use in clinical practice has had a major impact on the management of gastric cancer.(1) Histopathologic diagnosis remains the foundation of clinical decision making in the treatment of gastric neoplasia. However, based on subjective morphologic criteria, clinicians and pathologists continue to have concerns about the ability of pathologists to achieve consistent and accurate diagnoses using published criteria.(2) In 2000, a group of gastrointestinal pathologists convened in Vienna, Austria, for the purpose of developing a new system for the classification of dysplasia that would help to minimize the widely recognized discrepancies in morphological interpretation of gastric epithelial dysplasia (GED) and to reach consensus on the nomenclature.(3) However, modification of the nomenclature has not resolved the high level of intra- and interobserver variability with regard to the pathological classification of neoplasia and its mimickers. These interobserver variations are not a problem confined to Western and Japanese regions, and poor interobserver agreement in the distinction between high-grade dysplasia and adenocarcinoma in the pretreatment biopsies of Brrett's esophagus has been reported among pathologists practicing in the same institute located in United States, where Barrett's esophagus is one of the most common medical conditions.(4)
In Japan, gastric carcinoma is diagnosed on nuclear and structural criteria, even when invasion is absent according to the Western viewpoint.(5) This may also contribute to the relatively high incidence and good prognosis of gastric carcinoma in Japan compared to Western countries. In Korea, the terminology, definitions, and diagnostic criteria for GED are very heterogeneous.(6) As one of the pathologists working in a large volume hospital and handling a large number of gastric biopsy specimens, our experiences in the pathologic diagnosis of GED and carcinoma might help identify the differences between Korea and Japan.
Materials and Methods
In July 2008, to observe interobserver variation between two pathologists working in two different countries, KMK visited RK in Japan with her collection of gastric biopsy specimens with follow up information and that were associated with diagnostic difficulty. Without any knowledge of follow up or diagnosis by KMK, RK diagnosed the H&E slides of KMK's gastric biopsy specimens.
Results
The overall differences in the diagnosis of gastric biopsies are depicted in Table 1.
1. Regenerative atypia
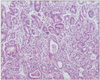
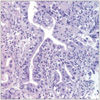
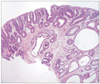
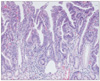
In the diagnosis of regenerative atypia, although we reached agreement in most cases (Fig. 1), we disagreed on two cases. One case (Fig. 2) diagnosed as regenerative atypia by KMK was diagnosed as suspicious carcinoma by RK and the other one diagnosed as favor reactive atypia was diagnosed as atypical glands with high-grade dysplasia by KMK (Fig. 3).
In cases that are difficult to diagnose, whether they are neoplasia, dysplasia or regenerative atypia, the Japanese guideline recommends making a temporary diagnosis of 'Group 2, indefinite for neoplasia'. This corresponds to 'Category 2' of the Vienna classification (Table 2).(7,8) In case of a 'Group 2' diagnosis, pathologists should comment on the reason for the diagnosis of 'indefinite for neoplasia', and, if possible, make 'deeper sections' or perform immunohistochemical stains for p53 and MIB-1. In those cases, Japanese pathologists sometimes use the term 'borderline lesion' or suspected adenocarcinoma for a biopsy case showing dysplastic lesions histologically beyond a typical tubular adenoma with low-grade dysplasia, and recommend endoscopic therapy. Even in a case of low-grade dysplasia, if the lesion shows predominantly gastric-foveolar type differentiation or villous/papillary structures, they prefer to make a diagnosis of 'suspicious of adenocarcinoma' rather than low-grade dysplasia. Such a lesion may invade into the submucosal layer, keeping its structure, without an invasive stromal reaction within the lamina propria.
2. GED (adenoma)
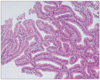
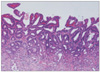
In the diagnosis of GED, we used "adenoma" in daily practice. There was general agreement on the diagnosis of adenoma with low-grade dysplasia. Glands in adenomas resembled colonic adenomas with crowded, tubular glands lined by atypical columnar cells with pencillate, hyperchromatic nuclei, with pseudostratification and inconspicuous nucleoli, mucin depletion, and lack of surface maturation.(3) Tumor glands show minimal architectural disarray and only mild to moderate cytological atypia and nuclei are located in the basal part of the glands (Fig. 4). However, several cases diagnosed as adenoma with low-grade dysplasia by KMK were diagnosed as adenoma with high-grade dysplasia by RK. For the diagnosis of adenoma with low-grade dysplasia, RK suggested that glands should be straight without branching, torsion and budding, and the nuclei should show spindling. However, KMK diagnosed adenoma with low-grade dysplasia based on criteria proposed by a study group of Korean gastrointestinal pathologists irrespective of glandular structural anomalies; the length of the nuclei should be lower than half of the height of the tumor cells and at least three contiguous glands should show these cytologic abnormalities.(9) In four cases diagnosed as adenoma with high-grade dysplasia, RK used the term "very well differentiated intramucosal intestinal type adenocarcinoma without invasion" (Fig. 5).
3. Adenocarcinoma
In cases diagnosed as invasive adenocarcinoma, distinct structural anomalies, such as marked glandular crowding, excessive branching, and budding were evident. Intraluminal necrotic debris was also common. Single tumor cells or clusters of them infiltrated within the lamina propria in the absence of desmoplasia. The neoplastic cells in intramucosal invasive neoplasia are usually cuboidal with a high nucleus to cytoplasm ratio. Round nuclei with prominent nucleoli and marked loss of polarity are common.(3) Mitoses are usually numerous and atypical mitoses can be identified. RK diagnosed adenocarcinoma in the absence of invasion into the lamina propria and thought that round oval nuclei found at the bottom or surface of foveolar epithelium with prominent nucleoli are adequate for the diagnosis of carcinoma. However, in cases with no definite invasion, KMK diagnosed them as adenoma with high-grade dysplasia (Fig. 6). This trend was more evident in histology when the tumor was gastric foveolar phenotype (Fig. 7). In Japan, the differential diagnosis between adenoma and adenocarcinoma is made on the basis of cellular and structural atypia. Even for small biopsy specimens, Japanese pathologists diagnose carcinoma if the tumor shows the same cellular and/or structural atypia as those of invasive carcinomas.
4. Adenocarcinoma in an adenoma
In the diagnosis of adenocarcinoma arising from an adenoma, RK used "adenocarcinoma associated with adenoma" when there was good circumscription of the carcinoma from the surrounding or adjacent adenoma, which shows clearly different histology from the carcinoma (Fig. 8A). In cases showing adenoma with high-grade dysplasia with gradual transformation to carcinoma, all tumor components were categorized as adenocarcinoma (not carcinoma in adenoma). If tumor cell nuclei shared the same morphology in areas of both invasive adenocarcinoma and non-invasive tumor, diagnosis of adenocarcinoma was made by RK. However, KMK diagnosed adenocarcinoma arising in adenoma in cases harboring definite areas of adenoma and showing transformation into invasive adenocarcinoma (Fig. 8B).
Conclusions
Although interobserver variation was present, it was not extreme and didn't affect treatment plans. However, diagnosing carcinoma on the basis of cellular and structural atypia, such as is done in Japan, may lead to a higher prevalence of gastric carcinoma and relatively good therapeutic results. Further international studies would help pathologists improve poor interobserver agreement in the distinction between high-grade dysplasia and adenocarcinoma.




 XML Download
XML Download