

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Crohn's disease (CD) is an immune-mediated chronic relapsing disorder that affects the gastrointestinal tract. International guidelines recommend that treatment of children with active luminal CD should follow a “step-up approach” [12].
First line induction therapy is either corticosteroids (to a maximum of 40 mg/day with gradual dose tapering) or exclusive enteral nutrition (for 6 to 8 weeks). Maintenance therapy is commonly started at the same time as induction therapy and includes standardized doses of mercaptopurine (1–1.5 mg/kg/day), azathioprine (2–2.5 mg/kg/day), or methotrexate (15 mg/m2/week). Anti-tumor necrosis factor (TNF) therapy in children with luminal CD is usually indicated after failure of conventional therapy or when immunosuppressive therapies are poorly tolerated.
Following the publication of major landmark randomized controlled trials that reported that infliximab (IFX) [3] and adalimumab (ADA) [4] can induce and maintain clinical remission in pediatric patients, the use of these medications has dramatically increased. Although these randomized controlled trials (RCTs) had high internal validity, their formal methodology puts severe constraints on the generalizability to real-world practice. Another drawback is that they had a relatively brief observation period with limited follow-up.
In contrast, observational (or real-world evidence) studies, may have greater generalizability to clinical practice because of the use of more diverse patient cohorts and generally longer follow-up periods. We aimed to determine the long-term efficacy of IFX and ADA in pediatric luminal CD by performing a systematic review of cohort studies.
MATERIALS AND METHODS
Eligibility criteria
Eligible studies were prospective and retrospective cohorts that followed patients for more than 1 year and reported time-to-event outcomes. Events were defined as a discontinuation of anti-TNF therapy for secondary loss of response. Secondary loss of response refers to patients who responded to induction therapy, but subsequently lost response during maintenance treatment. We accepted studies that recorded the Physician's Global Assessment (PGA) of disease activity, as well as studies that used the Pediatric Crohn's Disease Activity Index (PCDAI).
We narrowed our search to studies that exclusively included patients younger than 18 years and were published in English. Papers that were only presented in conferences in the form of an abstract, or those that exclusively focused on patients with perianal or fistulizing CD were excluded. Studies that evaluated the efficacy of anti-TNF agents after bowel resection were also excluded.
Information sources, identification, and selection of studies
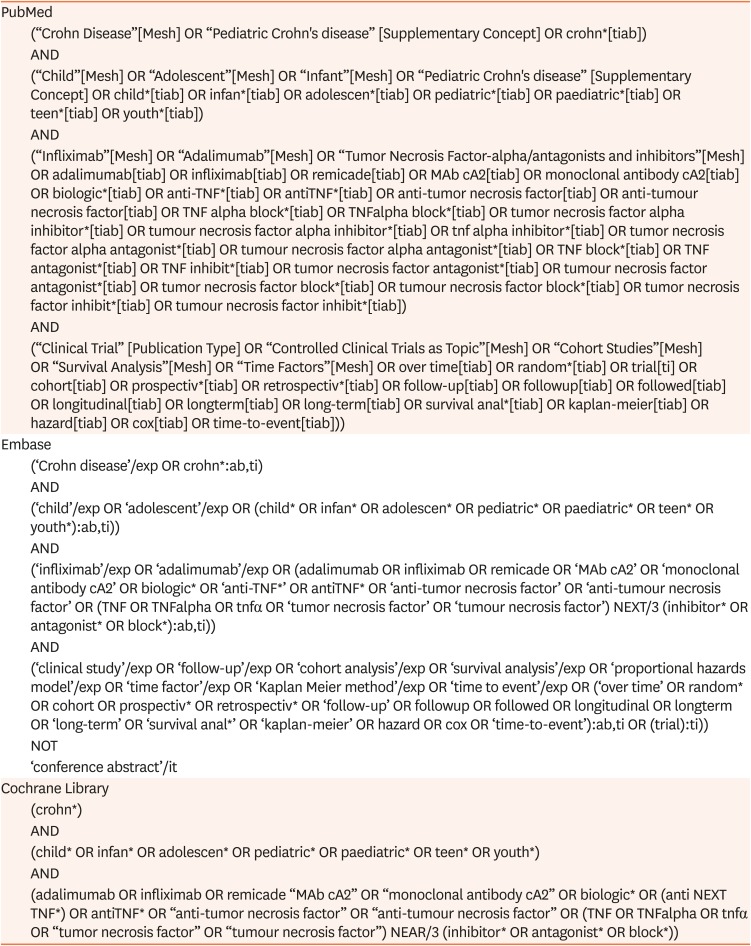
We searched for studies published in Medline, Embase, and the Cochrane Library from inception to September 26, 2019. The search strategies for each of the electronic databases are shown in Table 1.
Table 1
Search Strategy per Electronic Database From Inception to September 2019
The search results were imported into EndNote X9.2 for de-duplication [5], and subsequently imported in Rayyan, an online screening tool for systematic reviews [6]. One reviewer (HvR) performed the first selection of studies on the basis of title and abstract. The full text manuscript of each potentially eligible study was then obtained. Two authors (HvR and PFvR) independently appraised full text articles against the predefined inclusion criteria. Disagreements were resolved by discussion.
Data extraction
The following characteristics were extracted from each selected study: First author, year of publication, country of origin, cohort definition, observation period, median follow-up time, cohort size, age at study baseline, median time from diagnosis to start of study medication, reason for initiating anti-TNF, induction and maintenance scheme, application of dose escalation and interval shortening, and concomitant medication.
Finally, we extracted time-to-event curve data, as described by Tierney et al. [7] to estimate the probability of continuing biological therapy 1, 2, and 3 years after initiation of anti-TNF therapy. Pooling of time-to-event data was greatly jeopardized due to heterogeneity between studies and was therefore not performed.
RESULTS
Study selection
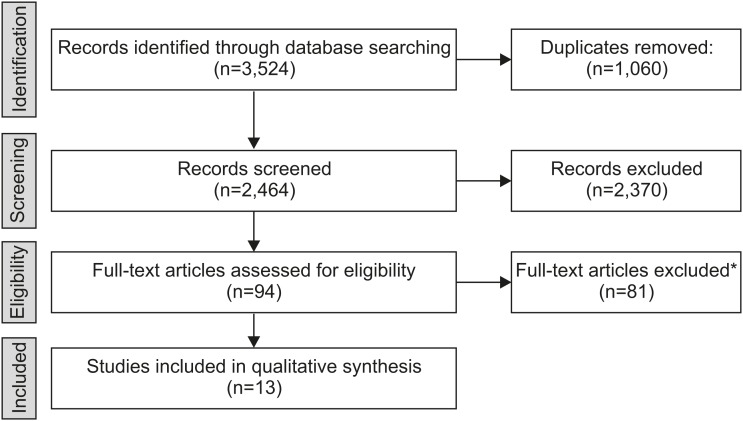
This review includes results of electronic searches up to September 26, 2019. In total, 2,464 study titles were screened, of which 94 were selected for full text review (Fig. 1) and 81 were excluded for not meeting the eligibility criteria. A total of 13 papers were ultimately included in the final analysis.
Fig. 1
Flow diagram of the systematic literature search. Reasons for exclusion at the last stage (*) included an observation period shorter than 1 year, adult patients, language other than English, case mix of ulcerative colitis and Crohn's disease, unacceptably high proportion lost-to-follow-up, no time-to-event analysis, randomized controlled trial or case-series, mix of infliximab and adalimumab therapy.
Study characteristics
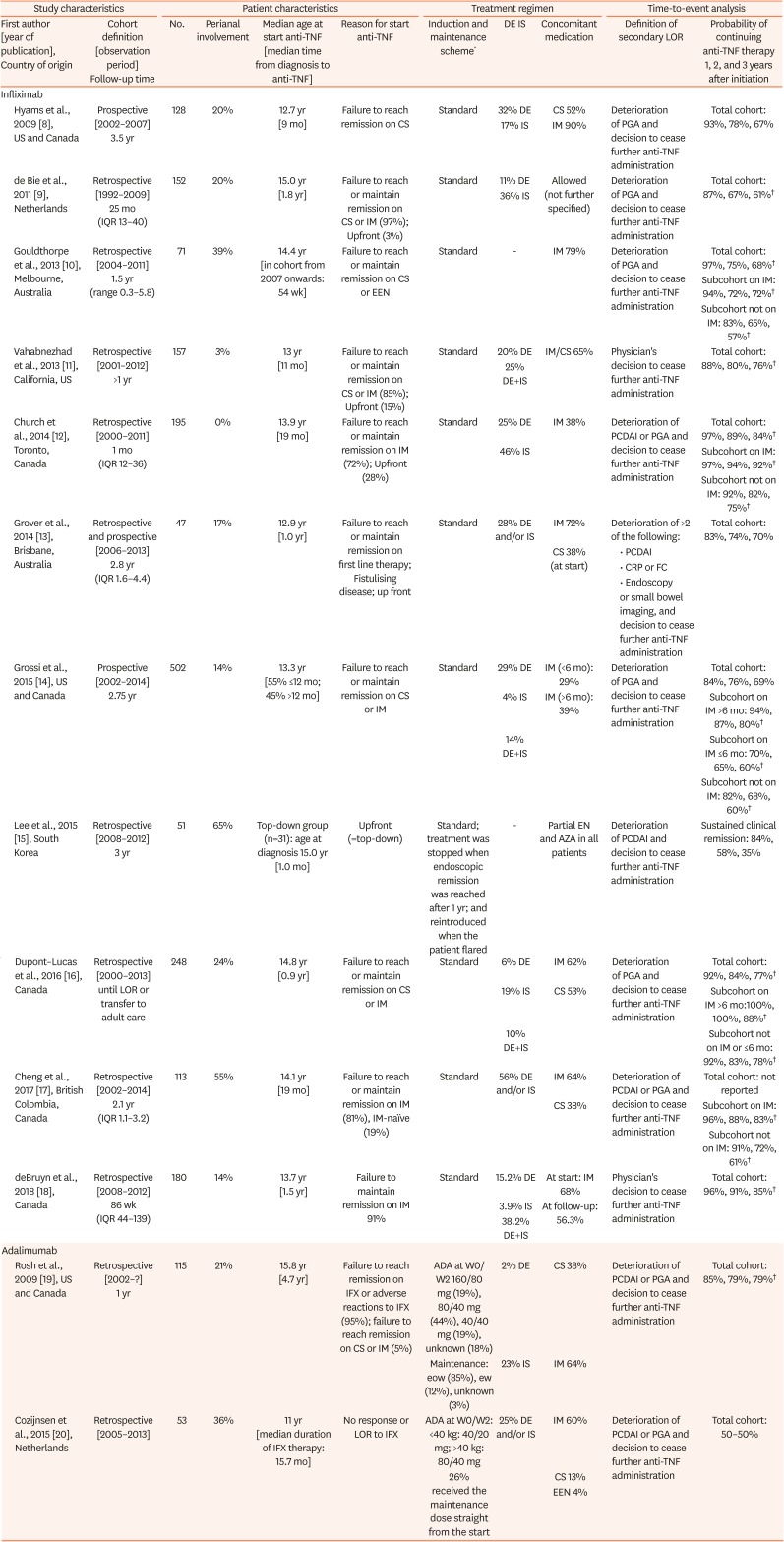
The study characteristics of the included studies are presented in Table 2. Eleven cohort studies evaluated patients who were following IFX therapy [89101112131415161718], while the other two studies described patients who were following ADA therapy [1920]. Two of the eleven studies on IFX had a prospective design [814], while the remainder were retrospective in nature [9101112
1315161718]. All studies were published in the last 10 years, and represent daily practices in North America, Europe, Australia, Israel, and South Korea. In one study, CD patients with perianal involvement were excluded from analysis [12], while in the other twelve studies, perianal involvement varied from 3% [11] to 65% [15]. The cohort size varied between 47 [13] and 502 patients [14], and the median observation period was 1.0 to 3.5 years. The median time from diagnosis to the start of IFX therapy was between 1 month [15] and 1.8 years [9], and from diagnosis to the start of ADA therapy was between 15.7 months [20] and 4.7 years [19]. Patients who received IFX therapy had not been previously exposed to anti-TNFs, while all patients who received ADA therapy had previously failed, or had experienced adverse reactions to, IFX [1920]. In ten cohort studies, a secondary loss of response was defined as a deterioration of PCDAI or PGA [891012141516171920]. In one study, a combination of clinical, biochemical, and endoscopic deterioration was used [13], and in two studies the reason to discontinue anti-TNF therapy was not specified [1118].
Table 2
Characteristics of included studies (n=13)
| Study characteristics | Patient characteristics | Treatment regimen | Time-to-event analysis | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First author [year of publication], Country of origin | Cohort definition [observation period] Follow-up time | No. | Perianal involvement | Median age at start anti-TNF [median time from diagnosis to anti-TNF] | Reason for start anti-TNF | Induction and maintenance scheme* | DE IS | Concomitant medication | Definition of secondary LOR | Probability of continuing anti-TNF therapy 1, 2, and 3 years after initiation | ||
| Infliximab | ||||||||||||
| Hyams et al., 2009 [8], US and Canada | Prospective [2002–2007] 3.5 yr | 128 | 20% | 12.7 yr [9 mo] | Failure to reach remission on CS | Standard | 32% DE | CS 52% | Deterioration of PGA and decision to cease further anti-TNF administration | Total cohort: 93%, 78%, 67% | ||
| 17% IS | IM 90% | |||||||||||
| de Bie et al., 2011 [9], Netherlands | Retrospective [1992–2009] 25 mo (IQR 13–40) | 152 | 20% | 15.0 yr [1.8 yr] | Failure to reach or maintain remission on CS or IM (97%); Upfront (3%) | Standard | 11% DE | Allowed (not further specified) | Deterioration of PGA and decision to cease further anti-TNF administration | Total cohort: 87%, 67%, 61%† | ||
| 36% IS | ||||||||||||
| Gouldthorpe et al., 2013 [10], Melbourne, Australia | Retrospective [2004–2011] 1.5 yr (range 0.3–5.8) | 71 | 39% | 14.4 yr [in cohort from 2007 onwards: 54 wk] | Failure to reach or maintain remission on CS or EEN | Standard | - | IM 79% | Deterioration of PGA and decision to cease further anti-TNF administration | Total cohort: 97%, 75%, 68%† | ||
| Subcohort on IM: 94%, 72%, 72%† | ||||||||||||
| Subcohort not on IM: 83%, 65%, 57%† | ||||||||||||
| Vahabnezhad et al., 2013 [11], California, US | Retrospective [2001–2012] >1 yr | 157 | 3% | 13 yr [11 mo] | Failure to reach or maintain remission on CS or IM (85%); Upfront (15%) | Standard | 20% DE | IM/CS 65% | Physician's decision to cease further anti-TNF administration | Total cohort: 88%, 80%, 76%† | ||
| 25% DE+IS | ||||||||||||
| Church et al., 2014 [12], Toronto, Canada | Retrospective [2000–2011] 1 mo (IQR 12–36) | 195 | 0% | 13.9 yr [19 mo] | Failure to reach or maintain remission on IM (72%); Upfront (28%) | Standard | 25% DE | IM 38% | Deterioration of PCDAI or PGA and decision to cease further anti-TNF administration | Total cohort: 97%, 89%, 84%† | ||
| 46% IS | Subcohort on IM: 97%, 94%, 92%† | |||||||||||
| Subcohort not on IM: 92%, 82%, 75%† | ||||||||||||
| Grover et al., 2014 [13], Brisbane, Australia | Retrospective and prospective [2006–2013] 2.8 yr (IQR 1.6–4.4) | 47 | 17% | 12.9 yr [1.0 yr] | Failure to reach or maintain remission on first line therapy; Fistulising disease; up front | Standard | 28% DE and/or IS | IM 72% | Deterioration of >2 of the following: | Total cohort: 83%, 74%, 70% | ||
| CS 38% (at start) | • PCDAI | |||||||||||
| • CRP or FC | ||||||||||||
| • Endoscopy | ||||||||||||
| or small bowel imaging, and decision to cease further anti-TNF administration | ||||||||||||
| Grossi et al., 2015 [14], US and Canada | Prospective [2002–2014] 2.75 yr | 502 | 14% | 13.3 yr [55% ≤12 mo; 45% >12 mo] | Failure to reach or maintain remission on CS or IM | Standard | 29% DE | IM (<6 mo): 29% | Deterioration of PGA and decision to cease further anti-TNF administration | Total cohort: 84%, 76%, 69% | ||
| 4% IS | IM (>6 mo): 39% | Subcohort on IM >6 mo: 94%, 87%, 80%† | ||||||||||
| 14% DE+IS | Subcohort on IM ≤6 mo: 70%, 65%, 60%† | |||||||||||
| Subcohort not on IM: 82%, 68%, 60%† | ||||||||||||
| Lee et al., 2015 [15], South Korea | Retrospective [2008–2012] 3 yr | 51 | 65% | Top-down group (n=31): age at diagnosis 15.0 yr [1.0 mo] | Upfront (=top-down) | Standard; treatment was stopped when endoscopic remission was reached after 1 yr; and reintroduced when the patient flared | - | Partial EN and AZA in all patients | Deterioration of PCDAI and decision to cease further anti-TNF administration | Sustained clinical remission: 84%, 58%, 35% | ||
| Dupont–Lucas et al., 2016 [16], Canada | Retrospective [2000–2013] until LOR or transfer to adult care | 248 | 24% | 14.8 yr [0.9 yr] | Failure to reach or maintain remission on CS or IM | Standard | 6% DE | IM 62% | Deterioration of PGA and decision to cease further anti-TNF administration | Total cohort: 92%, 84%, 77%† | ||
| 19% IS | CS 53% | Subcohort on IM >6 mo:100%, 100%, 88%† | ||||||||||
| 10% DE+IS | Subcohort not on IM or ≤6 mo: 92%, 83%, 78%† | |||||||||||
| Cheng et al., 2017 [17], British Colombia, Canada | Retrospective [2002–2014] 2.1 yr (IQR 1.1–3.2) | 113 | 55% | 14.1 yr [19 mo] | Failure to reach or maintain remission on IM (81%), IM-naïve (19%) | Standard | 56% DE and/or IS | IM 64% | Deterioration of PCDAI or PGA and decision to cease further anti-TNF administration | Total cohort: not reported | ||
| CS 38% | Subcohort on IM: 96%, 88%, 83%† | |||||||||||
| Subcohort not on IM: 91%, 72%, 61%† | ||||||||||||
| deBruyn et al., 2018 [18], Canada | Retrospective [2008–2012] 86 wk (IQR 44–139) | 180 | 14% | 13.7 yr [1.5 yr] | Failure to maintain remission on IM 91% | Standard | 15.2% DE | At start: IM 68% | Physician's decision to cease further anti-TNF administration | Total cohort: 96%, 91%, 85%† | ||
| 3.9% IS | At follow-up: 56.3% | |||||||||||
| 38.2% DE+IS | ||||||||||||
| Adalimumab | ||||||||||||
| Rosh et al., 2009 [19], US and Canada | Retrospective [2002–?] 1 yr | 115 | 21% | 15.8 yr [4.7 yr] | Failure to reach remission on IFX or adverse reactions to IFX (95%); failure to reach remission on CS or IM (5%) | ADA at W0/W2 160/80 mg (19%), 80/40 mg (44%), 40/40 mg (19%), unknown (18%) | 2% DE | CS 38% | Deterioration of PCDAI or PGA and decision to cease further anti-TNF administration | Total cohort: 85%, 79%, 79%† | ||
| Maintenance: eow (85%), ew (12%), unknown (3%) | 23% IS | IM 64% | ||||||||||
| Cozijnsen et al., 2015 [20], Netherlands | Retrospective [2005–2013] | 53 | 36% | 11 yr [median duration of IFX therapy: 15.7 mo] | No response or LOR to IFX | ADA at W0/W2: <40 kg: 40/20 mg; >40 kg: 80/40 mg | 25% DE and/or IS | IM 60% | Deterioration of PCDAI or PGA and decision to cease further anti-TNF administration | Total cohort: 50–50% | ||
| 26% received the maintenance dose straight from the start | CS 13% | |||||||||||
| EEN 4% | ||||||||||||
TNF: tumor necrosis factor, DE: dose-escalation, IS: interval shortening, LOR: loss of response, IQR: interquartile range, IFX: infliximab, CS: corticosteroids, IM: immunomodulator, EEN: exclusive enteral nutrition, ADA: adalimumab, EN: enteral nutrition, AZA: azathioprine, PGA: Physician's Global Assessment, PCDAI: Paediatric Crohn's Disease Activity Index, CRP: C-reactive protein, FC: faecal calprotectin.
*Standard induction and maintenance scheme is IFX (5 mg/kg) at W0, W2, and W6, then 8-weekly. †Probability data manually extracted from time-to-event curves.
Findings
1. Probability of continuing infliximab therapy at 1, 2, and 3 years
In ten of eleven studies, the indication to start IFX therapy was failure to reach remission on corticosteroids or exclusive enteral nutrition, or to maintain remission on immunomodulators. Upfront IFX therapy was evaluated in one group of Korean pediatric patients [15]. A starting dose of 5 mg/kg at weeks 0, 2, and 6 was the standard induction regimen in all studies, followed by subsequent 8-weekly infusions during the maintenance phase. Reactive dose escalations (up to 10 mg/kg) and/or interval shortening for secondary loss of response were performed in all but two studies. In an Australian study, [10] government regulations precluded a dose escalation, while in the Korean study [15] dose or interval adjustments were not mentioned.
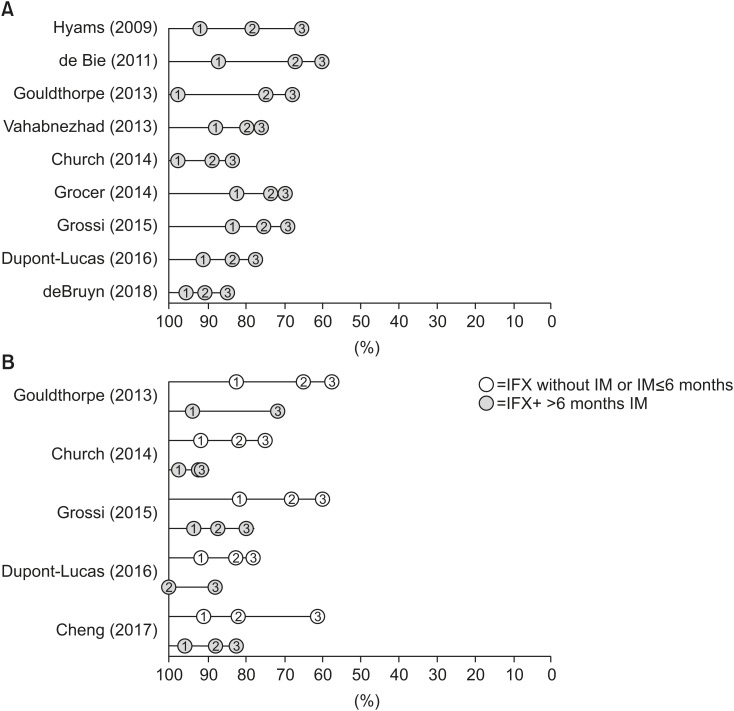
Fig. 2A shows that 1 year after the initiation of IFX therapy the probability of still receiving IFX was between 83% [13] to 97% [1012]. Two years after the initiation of IFX therapy the probability of still receiving IFX was between 67% [9] and 91% [18]. Three years after the initiation of IFX therapy the probability of still receiving IFX was between 61% [9] to 85% [18].
Fig. 2
Summary of probabilities of continuing infliximab at 1, 2, and 3 years after initiation. Plots display the probabilities of continuing infliximab therapy in included studies. The upper panel (A) shows the results of the entire cohort and the lower panel (B) shows the results of sub cohorts on either infliximab monotherapy or short combination therapy (white dots) vs. prolonged combination therapy (dark grey).
IFX: infliximab, IM: immunomodulator.
2. Probability of continuing infliximab therapy when combined with immunomodulator use
Five of eleven studies [1012141617] subgrouped their patients by concomitant immunomodulator use and consistently showed that the probabilities of continuing IFX therapy in patients with prolonged immunomodulator use (i.e. longer than 6 months) were higher than for patients on IFX monotherapy (Fig. 2B).
3. Probability of continuing adalimumab therapy at 1, 2, and 3 years
Almost all patients following ADA had previously been exposed to IFX. The ADA starting doses were weight-dependent, but there was no uniformity between the two studies. Dose escalation, interval shortening, and concomitant immunomodulator use were allowed in both studies. A year after initiation of ADA therapy the probability of still receiving ADA was between 50% [20] to 85% [19].
DISCUSSION
This review of real-world evidence studies confirms the long-term therapeutic benefit of anti-TNF agents in diverse cohorts of pediatric patients with luminal CD. The probability of still receiving IFX 3 years after initiation exceeded 50% in all cohort studies, despite the fact that the majority of patients had previously failed on first line induction or maintenance therapy. Patients with concomitant immunomodulator use for 6 months or longer had higher probabilities of continuing IFX therapy 3 years after initiation than patients on IFX monotherapy. This suggests that the durability of IFX is enhanced in combination therapy. The limited number of time-to-event studies in patients on ADA therapy prevented us from drawing definite conclusions about the long-term efficacy of ADA. The fact that the patients following ADA therapy had previously been exposed to anti-TNF implies that the long-term efficacy may be better in anti-TNF naive patients.
Comparison with other studies
We report the first systematic review to incorporate summary time-to-event data to evaluate the long-term efficacy of anti-TNF agents in pediatric CD. To date, there have been two systematic reviews on the short-term efficacy of anti-TNF agents in pediatric patients, one focusing exclusively on IFX [21] and a second exclusively on ADA [22].
Li and colleagues [21] included three RCTs and 19 prospective cohort studies comparing IFX with other therapies (including ADA and exclusive enteral nutrition), and defined induction of endoscopic remission by 14 weeks and maintenance of endoscopic remission at 6 months as their outcomes of interest. Dziechciarz and colleagues [22] were mainly interested in the proportion of patients with remission at 4 and 12 weeks after the first dose of ADA, and the proportion of patients who maintained remission throughout the first year. They included one RCT and 13 observational studies, which were classified as case series; among these studies, we considered two of these to be retrospective cohort studies [1920]. Similar to our study, they also concluded that there is a need for more high-quality evidence on the efficacy of ADA in pediatric CD.
Strengths and limitations
Although the current method provides a means of analyzing time-to-event outcomes for individual studies, it relies solely on published data for systematic reviews. For example, it was not possible to include all relevant studies because the outcome of interest was sometimes missing from the study report. Similarly, this method cannot correct for flaws in the design of the primary studies, such as post hoc exclusion of patients or failure to apply the intention-to-treat principle. In addition, different definitions of secondary loss of response may have affected the comparability of the outcome of interest between studies.
Despite these limitations, real-world evidence studies surely complement the findings from RCTs by providing valuable information on treatment practices and patient characteristics among unselected patients. When individual participant data (IPD) is unavailable, the analysis of time-to-event outcomes is an appropriate alternative.
Trough levels and antibody measurements were not routinely assayed in the studies under review, but rather on a reactive basis when patients had secondary loss of response. In a recently published RCT in pediatric patients with luminal CD, it was shown that proactive measurement of ADA trough levels improved treatment efficacy up to 72 weeks after initiation [23]. These findings are of importance to further optimize the durability of anti-TNF agents in children who are known to be underdosed when standard regimens are applied [24].
Implications for pediatric practice
The benefits of concomitant immunomodulator use must be balanced against the increased risks of prolonged combination therapy, particularly lymphoma risk with thiopurines. No such risk has been detected when low-dose methotrexate is administered once weekly as an immunomodulator. Stopping concomitant immunomodulation could be considered 6–12 months after initiation provided that IFX trough levels are in range and the patient is in clinical and biological remission.
Conclusion
This review of real-world evidence studies confirms the long-term therapeutic benefit of IFX therapy in children with luminal CD who failed first line therapies. Our findings suggest that combination therapy with an immunomodulator prolongs the durability of IFX therapy. More robust data on ADA therapy are necessary before we can draw definite conclusions about its long-term efficacy.
 XML Download
XML Download