

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute diarrhea is a common disease in children. The majority of cases are self-limited, requiring only conservative rehydration. However, acute infectious diarrhea can be clinically serious and is the second leading cause of death in children aged below 5 years, worldwide [12].
The major etiology of acute pediatric diarrhea is viruses. Rotavirus and pathogenic Escherichia coli are important causes of death due to infectious diarrhea [12]. Diarrheagenic bacteria including Clostridium difficile, Salmonella, Shigella, and Campylobacter cause invasive inflammation of the intestine, warranting extensive investigation and appropriate use of antimicrobial treatment [34]. Therefore, accurate and prompt laboratory testing for the differential diagnosis of bacterial versus viral infection in pediatric acute diarrhea may facilitate the prediction of the clinical course and timing of antimicrobial therapy [5].
Serum C-reactive protein (CRP) is an acute-phase reactant, and is utilized for the diagnosis and clinical follow-up of various inflammatory conditions including bacterial infection [67]. Several biomarkers derived from neutrophils in feces correlate strongly with gut inflammatory conditions such as Crohn’s disease or ulcerative colitis. These biomarkers include calprotectin (a calcium- and zinc-binding protein in neutrophils), lactoferrin (an iron-binding glycoprotein present in the secondary granules of neutrophils), myeloperoxidase (MPO), which is released from neutrophil primary granules, and polymorphonuclear elastase (PMN-e) found in neutrophil azurophilic granules [891011]. In particular, fecal calprotectin and lactoferrin are useful biomarkers in distinguishing gut pathogens in children with acute infectious diarrhea without underlying gut disease [481213]. In a previous study, we suggested that fecal lactoferrin was a useful marker for bacterial etiology in adult acute diarrhea, and that multiplex polymerase chain reaction (PCR) facilitated the detection of enteric pathogens [514]. However, limited evidence supports the clinical significance of various fecal biomarkers in acute pediatric gastroenteritis without underlying gut disease.
In this study, we evaluated the clinical significance of noninvasive fecal biomarkers including calprotectin, lactoferrin, PMN-e, and MPO together with blood inflammatory biomarkers including CRP, ESR, and leukocytes in pediatric acute diarrhea.
MATERIALS AND METHODS
This prospective study was approved by the Institutional Review Board of Incheon St. Mary's Hospital (IRB No. OC13TISI0014) in accordance with the ethical standards of the Declaration of Helsinki and written informed consents were obtained before the participants were enrolled. Between June 2013 and July 2014, children were enrolled according to the following criteria: age between 1 month and 18 years, acute diarrheal symptoms within 2 weeks, and admission due to diarrhea-associated moderate-to-severe dehydration, fever (≥38°C) or bloody diarrhea. Children with underlying gastrointestinal diseases including inflammatory bowel diseases, hospital-acquired diarrhea, and other chronic diseases requiring intensive care were excluded.
Inflammatory biomarkers
Blood samples and stool specimens were collected within 24 hours of admission. Blood inflammatory biomarkers including highly sensitive C-reactive protein (Beckman Coulter, Inc., Brea, CA, USA), erythrocyte sedimentation rate (ESR) (TEST-1; Alifax, Polverara, Italy), and leukocytes from complete blood count (CBC) (Sysmex, Kobe, Japan), and fecal inflammatory biomarkers including calprotectin (Ridascreen®; R-Biopharm, Darmstadt, Germany), lactoferrin (Abcam; Cambridge, UK), MPO (Abcam), and PMN-e (Abcam) were assessed quantitatively. Fecal leukocytes were examined using microscopy. An average number of leukocytes that was ≥1/high power field was considered positive. Fecal occult blood was examined by an immunochemical occult blood test (OC-Sensor Diana; Eiken Chemical Co., Ltd. Tokyo, Japan). A result that was ≥100 ng/mL was considered positive.
Diarrheagenic pathogen detection
Conventional stool culture using selective agars for Salmonella, Shigella, and Vibrio species was performed. Multiplex PCR for stool specimens was performed using the Seeplex® Diarrhea ACE detection kit (Seegene, Seoul, Korea) for the detection of four viruses (astrovirus, enteric adenovirus, group A rotavirus, and norovirus GI/GII), and 10 bacteria (Aeromonas spp., Campylobacter spp., C. difficile toxin B, Clostridium perfringens, E. coli O157:H7, verocytotoxin-producing E. coli (VTEC), Salmonella spp., Shigella spp., Yersinia enterocolitica, and Vibrio spp.). Fecal microscopic examination for intestinal protozoal parasites was also performed.
Statistics
Results are presented as median (range) or number (percentage). Categorical data were tested using the χ2 test or Fisher's exact test for small expected frequencies. Mann-Whitney U-test was used for continuous data. Statistical analysis was performed with SPSS version 13.0 (SPSS Inc., Chicago, IL, USA). Receiver operator characteristic (ROC) curve analysis was performed by MedCalc Statistical Software version 15.6.1 (MedCalc Software bvba, Ostend, Belgium; https://www.medcalc.org; 2015). A p-value ≤0.05 was considered statistically significant.
RESULTS
Patient demographics and clinical parameters
A total of 62 pediatric patients were included in this study. Clinical findings are summarized in Table 1. The median age of patients was 2 years (range, 1 month to 18 years). Forty-five patients (72.6%) were male. Chief complaints of all patients improved without complication at discharge. Fever, bloody diarrhea, diarrheagenic bacteria, and diarrheagenic viruses were included in clinical parameters. Fever was detected in 33 patients (53.2%) and bloody diarrhea in 19 patients (30.6%). Causative pathogens were detected using conventional cultures and multiplex PCR assays as follows: 18 bacteria were detected in 18 patients (29.0%), 43 viruses were detected in 40 patients (64.5%), and bacterial and viral coinfection was detected in 12 patients (19.4%). Enteric adenovirus (35%) was most prevalent, followed by norovirus (22%), Salmonella spp. (10%), and Campylobacter spp. (9%), group A rotavirus (4%), Aeromonas spp. (3%), astrovirus (1%), E. coli O157:H7 (1%), C. perfringens (1%), and C. difficile toxin B (1%) as shown in Fig. 1.
Table 1
Summary of clinical findings


Inflammatory biomarkers
The median values and ranges of inflammatory biomarkers in 62 pediatric patients are summarized in Table 2, and were as follows: 11.9 mg/L (0–178.0 mg/L) for CRP, 16 mm/hour (1–82 mm/hour) for ESR, and 10,300/µL (3,070–78,700/µL) for leukocytes. The inflammatory biomarker levels in feces were as follows: 282 µg/g (<30–1,800 µg/g) for calprotectin, 12.8 µg/mL (0–64.9 µg/mL) for lactoferrin, 4.2 ng/mL (0–14.9 ng/mL) for MPO, and 5 ng/mL (0–1,939 ng/mL) for PMN-e. Fecal leukocytes were detected in 15 patients (24.2%) and fecal occult blood was positive in 19 patients (30.6%).
Table 2
Summary of blood and fecal inflammatory biomarkers

Correlation between clinical parameters and inflammatory biomarkers
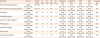
Of the nine blood and fecal inflammatory biomarkers, only CRP was significantly correlated with fever in pediatric acute diarrhea (p<0.001) (Table 3). CRP, ESR, fecal calprotectin, fecal lactoferrin, fecal MPO, fecal leukocytes, and fecal occult blood were significantly associated with bacterial pathogens in acute diarrhea (p<0.001, p=0.04, p=0.03, p=0.003, p=0.02, p=0.03, p=0.002, respectively). However, no inflammatory markers were found to correlate with viral pathogens in acute pediatric diarrhea (all, p>0.05).
Table 3
Correlation between clinical parameters and inflammatory biomarkers
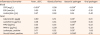
The area under the curve (AUC), the best cut-off values, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of the investigated parameters for bacterial infection are listed in Table 4. Among all the tested biomarkers, CRP showed the highest AUC (0.792), followed by fecal lactoferrin (0.739), fecal occult blood (0.715), fecal MPO (0.685), fecal calprotectin (0.675), ESR (0.674), and fecal leukocyte (0.643). Fecal calprotectin showed the highest sensitivity but the lowest specificity (38.6%) at the best cut-off value 74.0 µg/g (94.4%). Fecal leukocytes showed the highest specificity (84.1%) but lowest sensitivity (44.4%). Pairwise statistical comparison of ROCs among biomarkers showed no statistical significance (all, p>0.05).
Table 4
Diagnostic capability of tested biomarkers for bacterial infection in acute pediatric diarrhea (n=62)
Values are presented as number only, data (95% confidence interval), or percent only.
AUC: area under the curve, TP: true positive, FN: false negative, TN: true negative, FP: false positive, PPV: positive predictive value, NPV: negative predictive value, CRP: C-reactive protein, MPO: myeloperoxidase, ESR: erythrocyte sedimentation rate, HPF: high power field.
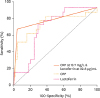
The combination of CRP and fecal lactoferrin showed the highest AUC (0.838) and accuracy (88.7%) for bacterial infection, which were higher than with individual biomarkers alone. The combination showed moderate sensitivity (72.2%) and high specificity (95.5%) (Table 4, Fig. 2). Pairwise statistical comparison of ROCs for the combination of CRP and fecal lactoferrin with ESR, lactoferrin, and calprotectin was as follows: p=0.011 for ESR, p=0.024 for lactoferrin, and p=0.006 for calprotectin, while comparison of ROCs for the combination of CRP and fecal lactoferrin with other biomarkers showed no statistical significance (all, p>0.05).
Fig. 2
Receiver operator characteristic plots of CRP, fecal lactoferrin, and the combination of CRP and fecal lactoferrin at their best cut-off values (CRP at 13.7 mg/L, lactoferrin at 22.8 μg/mL).
CRP: C-reactive protein.
The combination of CRP and fecal occult blood showed the highest specificity (100%) but low sensitivity (55.6%). Pairwise statistical comparison of ROCs for the combination of CRP and fecal occult blood with other biomarkers showed no statistical significance (all, p>0.05).
DISCUSSION
In this study, CRP, fecal lactoferrin, fecal leukocytes, and fecal occult blood were correlated with bacterial etiology in acute pediatric diarrhea. Among the biomarkers tested in this study, only CRP was correlated with both fever and bacterial etiology. Fecal occult blood was useful in determining bacterial etiology in pediatric acute diarrhea, but it was not a sensitive marker, which was in line with previous studies [515].
CRP at a cut-off value of 13.7 mg/L showed moderate diagnostic sensitivity (83.3%) and specificity (68.2%) with a 29% prevalence of bacterial diarrhea in this study. These results were similar to a prior study reported by Berger et al. [16] in which a CRP cut-off value of 20 mg/L showed a sensitivity of 83% and a specificity of 67% at a 24% prevalence of serious bacterial infections [17]. The findings are also in line with previous reports indicating that CRP has moderate sensitivity and specificity to detect bacterial infection in children with fever and can discriminate inflammatory from non-inflammatory diarrhea in young adults without underlying gastrointestinal diseases [1718].
Various fecal neutrophil-derived inflammatory biomarkers have been considered for noninvasive initial diagnosis and monitoring of inflammatory bowel disease in children [8910111920]. These biomarkers play a potential role in the assessment and diagnosis of various gastrointestinal conditions [20]. Although lactoferrin was less sensitive in determining the bacterial etiology of acute pediatric diarrhea than CRP in this study, it was better than the other fecal neutrophil-derived inflammatory biomarkers including calprotectin, MPO, and PMN-e. Most importantly, the combination of CRP and lactoferrin showed a higher diagnostic capability for bacterial etiology in acute pediatric diarrhea compared with their use alone. Therefore, lactoferrin may be used in conjunction with CRP in the differential diagnosis of bacterial infection in acute pediatric diarrhea without underlying gastrointestinal diseases.
There are several limitations in our study. First, the number of enrolled patients with bacterial diarrhea was relatively small because of the viral prevalence in childhood. Second, we failed to exclude all bacterial and viral pathogens in cases of acute diarrhea. Third, the positive PCR results may not represent the actual infectious status.
In summary, CRP is a useful marker for both fever and bacterial etiology in acute pediatric diarrhea. The combination of CRP and fecal lactoferrin has better diagnostic capability in ascertaining bacterial etiology than their use alone in acute pediatric diarrhea without underlying gastrointestinal diseases.
 XML Download
XML Download