

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ingestion of foreign bodies, particularly magnets, and their subsequent complications have become increasingly common with the majority occurring in children less than five years of age [1]. Data from the National Electronic Injury Surveillance System from 2002 to 2011 reveals an estimated 16,386 children presented to emergency centers in the United States with possible magnet ingestions [2]. During this 10-year period, the magnitude of magnetic ingestions by children has increased eight-and-a-half fold [2]. Increased frequency and morbidity have been noted specifically with the use of neodymium magnets. Neodymium magnets are high-powered, rare-earth magnets that exhibit over five times the force of traditional magnets, and have “demonstrated the tendency to cause gastrointestinal (GI) injury much more readily than their conventional counterparts” [3]. This poses a significant threat of possible bleeding, perforation, and enteroenteric fistulae when ingested, which often requires surgical intervention [4]. We report the case of a 19-month-old who ingested 13 neodymium magnets, which created a gastroduodenal fistula. These high-powered, rare-earth magnets created a significant gastroduodenal fistula, which was successfully treated with endoscopic removal and supportive care, avoiding the need for surgery.
CASE REPORT
A 19-month-old male in his usual state of good heath presented with a three-month history of progressive non-bloody, non-bilious emesis. The mother denied history of fever, diarrhea, or abdominal pain. His growth parameters plotted above the 75th percentile for height and weight, and there was no previous history of gastroesophageal reflux symptoms. He was referred to our institution where an upper GI series (UGI) showed 13 ingested foreign bodies connected end-to-end and looped from the stomach through the pylorus into the duodenum (Fig. 1). His mother reported that he had received a box of plastic colored magnets as a gift several months earlier.
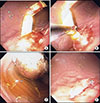
He was brought to the operating room where emergent endoscopy revealed that the most proximal, red-colored neodymium magnet in the stomach was magnetized to the anterior wall of the stomach (Fig. 2). Attempts to grasp the magnet with forceps were unsuccessful. The gastric foreign body had tightly adhered to the most distal, yellow-colored neodymium magnet located in the small intestine adjacent to the stomach. The forceps could not separate the magnets due to the strong magnetic attraction. A loop snare was inserted between the magnets and the proximal, red-colored magnet was tightly grasped. Significant force was applied to separate the proximal magnet from the wall of the stomach; however, this only led to the emergence of the distal, yellow- colored magnet from the small intestine through the gastric lumen (Fig. 2). This raised the possibility of intestinal perforation. Pediatric surgery was consulted intraoperatively. After much discussion, the decision was made to continue attempts at endoscopic removal prior to considering surgical exploration, as the patient remained clinically stable with a benign abdominal examination.
The proximal magnet was once again tightly grasped with the loop snare and drawn closely to the tip of the scope for better control (Fig. 2). In one smooth motion, the endoscope was torqued in a clockwise fashion and quickly withdrawn with some force. This separated the proximal gastric magnet from the distal small bowel magnet. The magnets were withdrawn through the mouth, magnetized to one another in linear fashion. Repeat endoscopic inspection of the area revealed a gastroduodenal fistula (Fig. 3), but no evidence of perforation.
The patient was admitted to the hospital for observation. He was given nothing by mouth and started on prophylactic intravenous antibiotics while pediatric surgery remained consulted. Follow-up 3-view abdominal films showed no evidence of perforation. He did not develop signs or symptoms of peritonitis. The patient did well during his hospitalization. His diet was gradually advanced as tolerated, and he was discharged home after three days of observation. The patient did well clinically and remained asymptomatic at his outpatient clinic visit two weeks later. Follow-up UGI six months later showed no evidence of a persistent gastroduodenal fistula.
Informed patient consent was obtained for publication of the case details.
DISCUSSION
Foreign body ingestions pose a significant health risk to the pediatric population. High-powered magnet ingestions, in particular, are challenging clinical cases for pediatric gastroenterologists. These types of ingestions are particularly difficult due to their insidious presentation and high risk of complications. The ingestion is often unwitnessed and associated symptoms can be nonspecific. Initially, ingestion of multiple magnets may not produce physical examination findings [5]. Furthermore, there is a paucity of clinical data in the form of prospective studies to guide management of these patients. A single magnet may pass without complications; however, multiple magnets usually require either endoscopy or surgical intervention [4]. In the presence of multiple magnets, there is the potential for significant morbidity and mortality. These include fistula formation, intestinal obstruction, perforation, peritonitis, bowel ischemia, pressure necrosis and death [6].
According to the most recent guidelines released in 2015 by the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN), urgent endoscopic removal is recommended in the presence of more than one magnet, even in asymptomatic patients [3]. If the magnets are lodged within the esophagus or stomach for less than 12 hours, then pediatric gastroenterology should be consulted. If the magnets have been present for greater than 12 hours, then consulting pediatric surgery is recommended prior to endoscopic removal. Once the magnets proceed beyond the pylorus, surgical intervention either by laparoscopy or laparotomy, is strongly recommended [4].
In the literature, there are few reported cases of fistula managed successfully with endoscopic removal alone. Hwang et al. [7] report a case of gastro-gastro-duodenal fistula formation in a 12-year-old male with autism following ingestion of twenty-two magnets. The magnets were removed by polypectomy snare and the patient was treated with two-week course of proton-pump inhibitors. Follow-up endoscopy revealed resolution of the fistulas. Ohno et al. [8] also describe a case of gastroduodenal fistula in a 7-year-old autistic child that was successfully removed endoscopically one week after ingestion.
In our patient's case, there were several indications in favor of endoscopic management in lieu of surgery. First and foremost, the chronicity of our patient's presenting symptoms in the absence of fever, weight loss, or alteration in bowel pattern suggests that the patient was a candidate for a less urgent approach. According to Sugawa et al. [9], “surgical management is recommended if severe abdominal pain develops.” Those without signs of obstruction or acute distress can be handled less urgently. Our patient had a benign abdominal examination and stable vital signs at the time of presentation. The absence of abdominal pain or distension in our patient made it less likely that complications such as bowel ischemia, obstruction, perforation, or peritonitis were present. Review of the literature suggests in the setting of multiple magnet ingestion, laparotomy should be considered “if signs of intestinal distress develop” and “if the magnetic beads have passed the pylorus and cannot be retrieved via endoscopy” [10]. In our patient's case, the magnets were endoscopically retrievable using a loop snare, which successfully removed all but one magnet. Lastly, the abdominal imaging that was obtained did not show subcutaneous air, pneumomediastinum, free air under the diaphragm, or other radiologic signs that would support that the patient had a bowel perforation that would warrant a more invasive approach such as surgery.
Our case highlights a well-known phenomenon that high-powered, rare earth magnet ingestion can lead to life-threatening complications. There is a need for a high index of suspicion for enteral fistula formation, especially following neodymium magnet ingestion [4]. Our patient's case also provides an example of a gastroduodenal fistula successfully treated with endoscopic removal and supportive care, avoiding the need for surgery.


 XML Download
XML Download