

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Multimatrix mesalazine (Lialda® in the United States; Mezavant™ XL in the United Kingdom, Ireland, and Malta; Mezavant™ elsewhere in the European Union) is a once daily (QD) oral formulation of mesalazine, the efficacy of which in mildly to moderately active UC has been demonstrated in 2 placebo-controlled studies.1
2 Since it has been reported that the therapeutic effect of oral mesalazine correlates with its concentration in the colonic mucosa,3 a higher dose of oral mesalazine should confer a greater clinical benefit. However, no apparent dose-response relationship was detected between 2 doses of multimatrix mesalazine (2.4 g/day and 4.8 g/day) in the above-mentioned placebo-controlled studies.
This study was conducted in patients with mildly to moderately active UC to investigate the efficacy and safety of 2 different doses of multimatrix mesalazine (2.4 g/day and 4.8 g/day), compared with time-dependent (controlled-release) mesalazine 2.25 g/day 3 times daily (TID) as an active comparator.
METHODS
1. Patients
Eligible participants were outpatients diagnosed with UC and aged ≥16 years, with a UC disease activity index (UC-DAI) score ≤4 and ≤10 at randomization assignment, sigmoidoscopy score ≥1, rectal bleeding score ≥1, and physician's global assessment (PGA) score ≤2. The UC-DAI consists of the following 4 variables: stool frequency, rectal bleeding, sigmoidoscopic findings regarding the mucosal appearance, and PGA. The UC-DAI employs a 4-point scoring scale from 0 to 3 to evaluate each variable, and the evaluation index score is the total of the 4 variables.4 Patients were excluded from the study if they had any of the following: history of hypersensitivity to mesalazine and salicylic acid; severe UC; chronic continuous or acute fulminating UC; use of oral mesalazine preparations >2.4 g/day or oral salazosulfapyridine preparations >4.0 g/day, topical mesalazine, topical salazosulfapyridine, adrenal corticosteroid or cytapheresis therapy within 2 weeks before randomization assignment, treatment with an immune-regulating drug or anti-tumor necrosis factor-α antibody within 12 weeks before randomization assignment; previous colonic resection (excluding appendectomy); moderate to severe renal or liver disorders; serious complications including diseases of the blood, respiratory, gastrointestinal, or cardiovascular organs; neuropsychiatric disease; metabolic/electrolyte imbalance or hypersensitivity; or malignant tumor. The following patients were also excluded: women who were pregnant, breastfeeding, or possibly pregnant; female patients who were planning to get pregnant during the study period.
2. Study Drugs
Multimatrix mesalazine tablets (Lialda®; Shire US Inc., Wayne, PA, USA) are red-brown, oval, film-coated tablets containing 1.2 g of mesalazine per tablet. The comparator, time-dependent (controlled-release) mesalazine tablets (Pentasa®; Kyorin Pharmaceutical Co., Ltd., Tokyo, Japan), are white to pale yellow uncoated tablets with grayish-white to pale grayish-yellow maculae containing 250 mg of mesalazine per tablet. The study adopted a double-dummy trial design. Adherence to each study drug was measured based on patient diaries.
3. Study Design
This was a multicenter, randomized, double-blind, active-controlled, and parallel-group study with an 8-week treatment period conducted at 56 study centers in Japan from January 2011 to May 2012 (Japan Pharmaceutical Information Center clinical trial registration number: Japic CTI-101380). After informed consent was obtained, patient eligibility was evaluated based on the inclusion/exclusion criteria, and the study drug was administered to eligible patients. The following 3 groups were given the study drugs: the multimatrix mesalazine 2.4 g/day QD (Multimatrix-2.4) group, the multimatrix mesalazine 4.8 g/day QD (Multimatrix-4.8) group, and the time-dependent (controlled-release) mesalazine 2.25 g/day TID (Time-2.25) group. Patients were randomized to 1 of the 3 groups in a 1:1:1 ratio by the permuted block method, with each study center as 1 block. A double-dummy design was adopted to maintain blinding of the investigators and study participants. The Multimatrix-2.4 group received 2 tablets of multimatrix mesalazine 1.2 g and 2 tablets of multimatrix mesalazine placebo after breakfast. The Multimatrix-4.8 group received 4 tablets of multimatrix mesalazine 1.2 g after breakfast. Both multimatrix groups received 3 tablets of controlled-release mesalazine placebo after each meal. The Time-2.25 group received 4 tablets of multimatrix mesalazine placebo after breakfast and 3 tablets of controlled-release mesalazine 250 mg after each meal.
4. Efficacy and Safety Evaluation
During the study, patients were required to visit the study center at weeks 2, 4, and 8. At each visit, efficacy and safety were evaluated by the investigator. The mean scores of daily stool frequency and rectal bleeding for 3 days before each visit were calculated based on the patient diary in which patients recorded stool frequency and rectal bleeding status. Colonoscopy was performed at the start of the treatment period and at week 8 or at the time of discontinuation, and the sigmoidoscopy score was assessed by the same investigator, with reference to the atlas of mucosal apperarance.5 The PGA score was evaluated based on the clinical symptoms and endoscopic findings at the beginning of the treatment period and at week 8 or at the time of discontinuation.
Adverse events (AEs) and vital signs were evaluated at each visit. Body weight and clinical laboratory test results were evaluated every 4 weeks or at the time of discontinuation. AEs were summarized by preferred term using the Medical Dictionary for Regulatory Activities version 15.0.
5. Objective/Endpoints
The primary objective of the efficacy evaluation was to demonstrate the non-inferiority of Multimatrix-2.4 to Time-2.25 and the superiority of Multimatrix-4.8 to Time-2.25 based on the primary efficacy endpoint, which was the change in the UC-DAI score from baseline to the end of the treatment period. The primary safety objective was to evaluate the AEs associated with the 3 treatments during the treatment period.
The secondary efficacy endpoints were: remission (UC-DAI score ≤2 and rectal bleeding score=0 at the end of the treatment period), clinical remission (rectal bleeding score=0 and stool frequency score=0 at the end of the treatment period), endoscopic remission (sigmoidoscopy score=0 at the end of the treatment period), improvement (from baseline, a decrease of at least 2 points in the UC-DAI score at the end of the treatment period), and the change in the score of each variable of the UC-DAI (score at the end of the treatment period-score at baseline). The secondary safety endpoints were adverse drug reactions (side effects) in the treatment period.
6. Statistical Analysis
The full analysis set (FAS) consisted of enrolled patients who received the study drug at least once and received a minimum of 1 efficacy evaluation. The per protocol set (PPS) was the primary analysis set for the efficacy analysis and consisted of patients in the FAS that satisfied the inclusion criteria and did not fall under any exclusion criteria, did not receive prohibited concomitant drugs or therapy, and had a drug adherence of ≥75%. The safety analysis set consisted of patients that received the study drug at least once and underwent safety assessment.
For primary analysis of efficacy, analysis of covariance, using the baseline UC-DAI score as a covariate, was performed on the change in the UC-DAI score, and the two-sided 95% CI of the difference between Multimatrix-2.4 and Time-2.25 was calculated in the PPS to evaluate non-inferiority. The non-inferiority margin (Δ) was set at 1.0 with respect to the change in the UC-DAI score according to previous non-inferiority studies.6
7 Only if non-inferiority was met, the superiority of Multimatrix-4.8 to Time-2.25 to be investigated in the FAS with a closed testing procedure. With remission, clinical remission, endoscopic remission, and improvement as secondary endpoints, the proportions of patients who achieved each endpoint in the Multimatrix-2.4 and Multimatrix-4.8 groups were compared to the proportions of patients that did so in the Time-2.25 group, along with the two-sided 95% CI of the difference. The changes in each variable of the UC-DAI were analyzed in the same manner as the primary endpoint. Subgroup analyses were performed to support the primary endpoint. For the safety endpoint, the incidence of AEs was compared among the treatment groups.
SAS version 9.2 (SAS Institute, Cary, NC, USA) was used for statistical analysis. Assuming that the difference in the UC-DAI score between Multimatrix-2.4 and the Time-2.25 was −0.5 and the difference in the UC-DAI score between Multimatrix-4.8 and Time-2.25 was −1.6 based on previous studies,2
6 and the SD was 3.0 in each group, we set the number of patients needed to demonstrate the non-inferiority of Multimatrix-2.4 to Time-2.25 and the superiority of Multimatrix-4.8 to Time-2.25 at 76 patients per group with a one-sided type 1 error (α) of 2.5%, with a power of more than 80% and Δ of 1.0.
7. Ethical Considerations
The study was conducted in accordance with ethical principles that have their origin in the Declaration of Helsinki; the Ministerial Ordinance on Good Clinical Practice for Drugs; and other relevant laws, regulations, and standards. Written informed consent was obtained from each patient. Prior to commencement of the study, the study protocol, a sample case report form, the patient information sheet, and informed consent form were approved by the Institutional Review Board at each study center; the appropriateness of the conduct of the clinical trial was also approved.
RESULTS
1. Patient Disposition and Baseline Characteristics
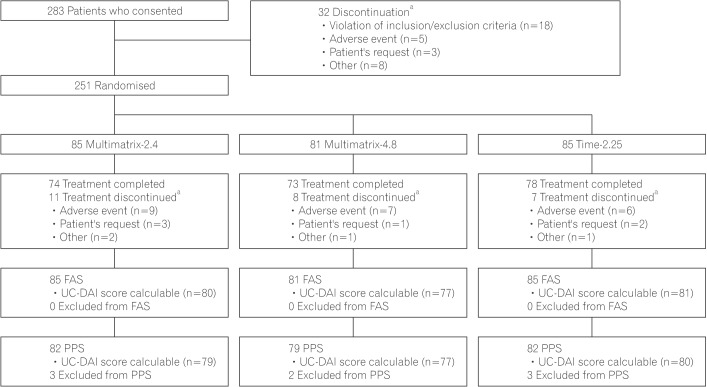
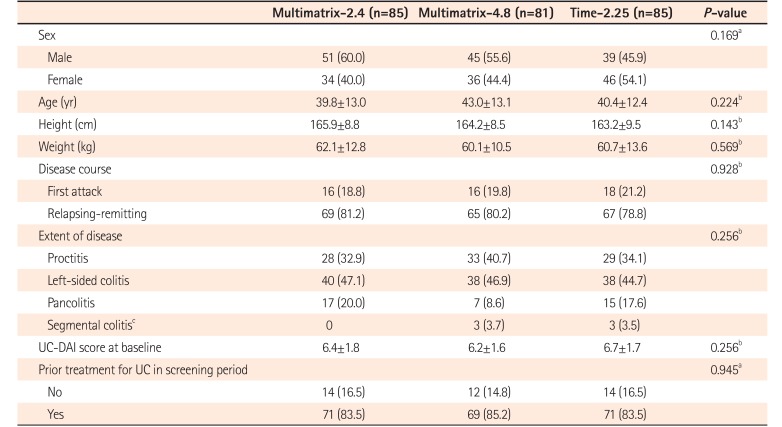
Patient disposition is shown in Fig. 1. Consent was obtained from 283 patients, and 251 received study drugs (Multimatrix-2.4, 85; Multimatrix-4.8, 81; Time-2.25, 85). Thirty-two patients withdrew from the study before the randomization assignment. Of the 251 patients who received the study drug, 225 patients completed treatment, and 26 patients (Multimatrix-2.4, 11; Multimatrix-4.8, 8; Time-2.25, 7) discontinued during the treatment period. The main reason for discontinuation in all treatment groups was AEs (Multimatrix-2.4, 9; Multimatrix-4.8, 7; Time-2.25, 6). The disposition of the FAS and PPS is shown in Fig. 1. No patients were excluded from the FAS. Eight patients were excluded from the PPS (Multimatrix-2.4, 3; Multimatrix-4.8, 2; Time-2.25, 3). The most common reason for exclusion from the PPS was failure to meet inclusion/exclusion criteria. Thirteen patients in the FAS had a change in the UC-DAI score that was not calculable (Multimatrix-2.4, 5; Multimatrix-4.8, 4; Time-2.25, 4). Seven patients in the PPS had a change in the UC-DAI score was not calculable (Multimatrix-2.4, 3; Multimatrix-4.8, 2; Time-2.25, 2). The mean rates of drug adherence in the PPS were not less than 95% in all treatment groups. There were no intergroup differences in terms of patient background factors in the FAS (Table 1).
2. Efficacy
1) Primary Endpoint
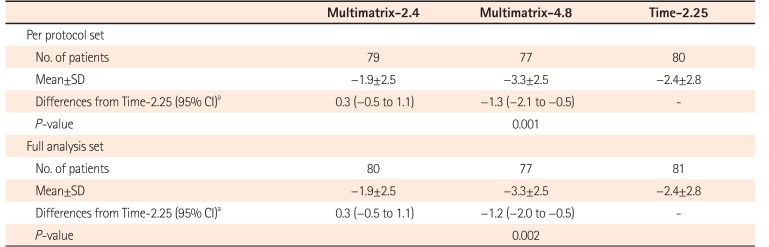
In the PPS, the change in the UC-DAI score at the end of the treatment period (mean±SD) was −1.9±2.5 in the Multimatrix-2.4 group, −3.3±2.5 in the Multimatrix-4.8 group, and −2.4±2.8 in the Time-2.25 group. The difference in the mean change in the UC-DAI score (adjusted) between the Multimatrix-2.4 group and the Time-2.25 group was 0.3 (two-sided 95% CI, −0.5 to 1.1). The upper limit of the two-sided 95% CI of the difference between the treatment groups was not lower than the non-inferiority margin (1.0), indicating that non-inferiority was not met (Table 2). Under the closed testing procedure adopted in this study, since the non-inferiority of the Multimatrix-2.4 group to the Time-2.25 group was not demonstrated, no further attempts were made to show if Multimatrix-4.8 was superior to Time-2.25. In the FAS, the change in the UC-DAI score at the end of the treatment period (mean±SD) was −1.9±2.5 in the Multimatrix-2.4 group, −3.3±2.5 in the Multimatrix-4.8 group, and −2.4±2.8 in the Time-2.25 group. In the ad hoc analysis where multiplicity was not taken into consideration, the difference in the UC-DAI score (adjusted) between the Multimatrix-4.8 group and the Time-2.25 group in the FAS was −1.2 (two-sided 95% CI, −2.0 to −0.5), which was statistically significant (Table 2).
2) Secondary Endpoints
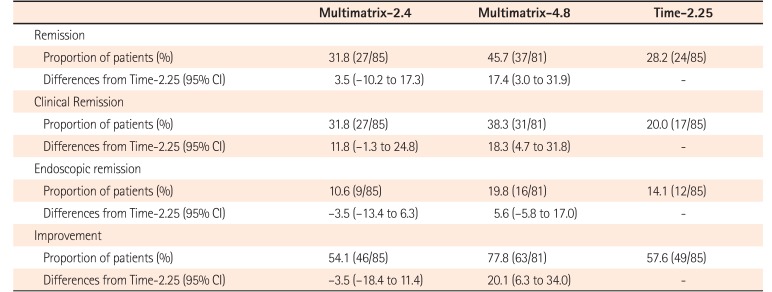
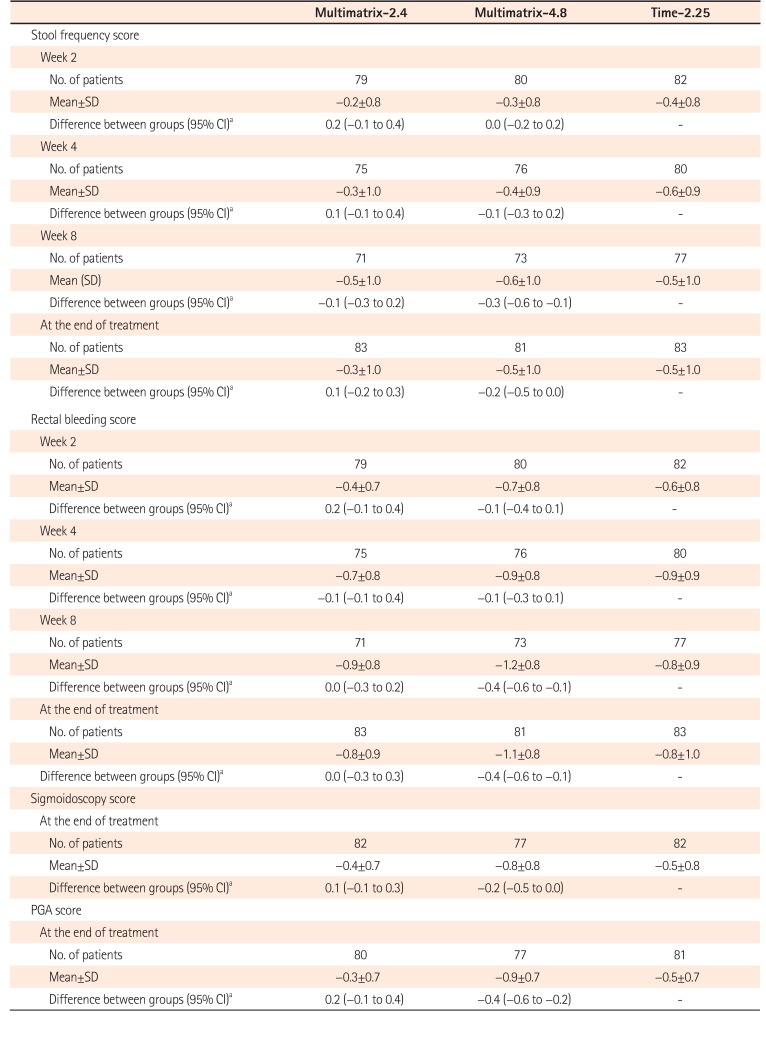
The proportions of patients who achieved remission, clinical remission, endoscopic remission, and improvement are shown in Table 3. The proportions of patients who achieved each endpoint were similar between the Multimatrix-2.4 group and the Time-2.25, and a greater proportion of patients in the Multimatrix-4.8 group achieved each endpoint than in the Time-2.25 group. The change in the UC-DAI by variable is shown in Table 4. A decrease was observed in both the rectal bleeding score and the stool frequency score from week 2 in in all 3 treatment groups. The sigmoidoscopy score and the PGA score had also improved from baseline by the end of treatment. Generally, the results of the Multimatrix-2.4 group and the Time-2.25 group appeared to be similar, and the Multimatrix-4.8 group showed greater improvement compared with the other 2 groups for all secondary endpoints.
3) Subgroup Analysis
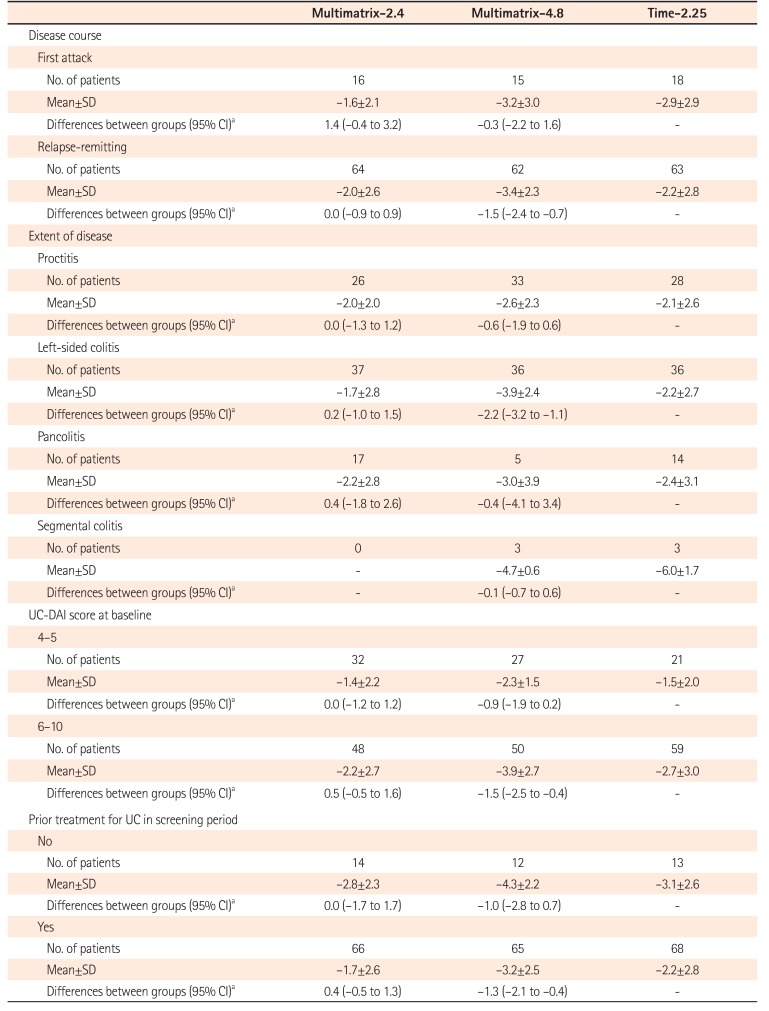
The results of subgroup analyses for the primary endpoint are shown in Table 5. Concerning the main UC categories (classification by disease course, extent of disease, UC-DAI score at baseline), the Multimatrix-4.8 group showed a trend towards greater improvement in the UC-DAI score than the Time-2.25 group in all subgroups (Table 5).
3. Safety
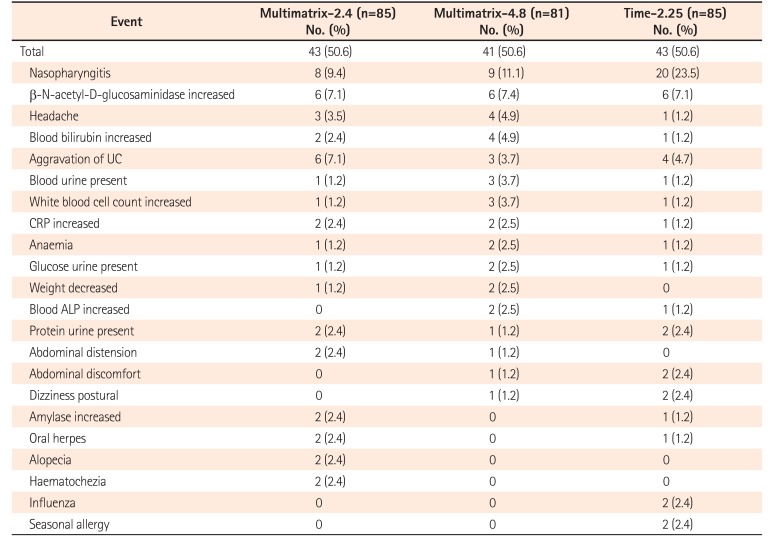
The incidence of AEs (proportion of patients who experienced at least 1 AE) during the treatment period was 50.6% (43/85 patients) in the Multimatrix-2.4 group, 50.6% (41/81 patients) in the Multimatrix-4.8 group, and 50.6% (43/85 patients) in the Time-2.25 group (Table 6). The most common AEs (more than 5% incidence in any treatment group) were nasopharyngitis, increase in N-acetyl-beta-D-glucosaminidase, and aggravation of UC. The incidence of these AEs in individual treatment groups is shown in Table 6. The incidence of adverse drug reactions (side effects) during the treatment period was 24.7% (21/85) in the Multimatrix-2.4 group, 27.2% (22/81) in the Multimatrix-4.8 group, and 18.8% (16/85) in the Time-2.25 group.
There were no deaths during the course of the study. Concerning serious AEs during the treatment period, aggravation of UC occurred in 1 patient in the Multimatrix-2.4 group, while aggravation of UC and headache occurred in 1 patient each in the Multimatrix-4.8 group. All of these events were adverse drug reactions. No serious AEs occurred in the Time-2.25 group. During the follow-up period, pericarditis occurred in 1 patient in the Multimatrix-4.8 group. No causal relationship was found between the events and the study drugs.
DISCUSSION
The primary objective of this study was to demonstrate the non-inferiority of Multimatrix-2.4 to Time-2.25, but this was not achieved. It is possible that the failure to demonstrate the non-inferiority could be attributed to the fact that the sample size was determined under the assumption that the difference in change in UC-DAI score between Multimatrix-2.4 and Time-2.25 was −0.5, although actual the difference between 2 groups was found to be 0.3. We estimated the difference between Multimatrix-2.4 to Time-2.25 in the present study based on the results of the 2 previous studies. One was a placebo-controlled study which compared multimatrix mesalamine 2.4 g/day, 4.8 g/day, placebo, and pH-dependent release mesalazine 2.4 g/day as a reference arm, in which the difference in the change in UC-DAI score between multimatrix mesalamine 2.4 g/day and pH-dependent release mesalazine 2.4 g/day was 0.24.2 The other was a study which compared pH-dependent release mesalazine 2.4 g/day, 3.6 g/day, time-dependent release mesalamine 2.25 g/day, and placebo, in which the difference in the change in UC-DAI score between pH-dependent release mesalazine 2.4 g/day and time-dependent release mesalamine 2.25 g/day was 0.2.6 Based on these results, we estimated the difference between Multimatrix-2.4 and Time-2.25 to be 0.5, but this resulted in the efficacy of Multimatrix-2.4 being overestimated. However, considering the results for the secondary endpoints, Multimatrix-2.4 appeared to have comparable efficacy to that of Time-2.25. This finding is supported by a previous study in which the efficacy of multimatrix mesalazine 2.4 g/day QD was comparable to a similar dose of Asacol tablets 2.4 g/day TID.2
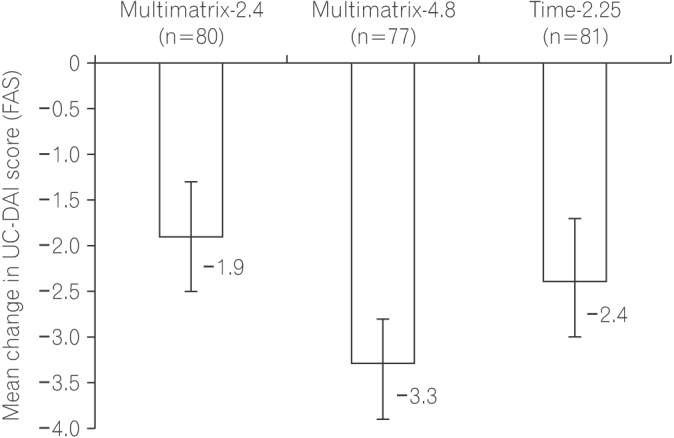
In the present study, the mean change in UC-DAI score and two-sided 95% CI in the FAS was −3.3 (−3.9 to −2.8) in the Multimatrix-4.8 group and −1.9 (−2.5 to −1.3) in the Multimatrix-2.4 group (Fig. 2), indicating that multimatrix mesalazine 4.8 g/day is more effective than 2.4 g/day. However, in the previous placebo-controlled studies of multimatrix mesalazine, no dose-response relationship was detected between the 2 doses (2.4 g/day and 4.8 g/day).1
2 In these studies, patients were permitted to use oral mesalazine at a dose of 2.0 g/day or less if they were receiving this therapy prior to screening. In another report, which assessed the efficacy of multimatrix mesalazine in various patient subgroups using patients pooled from these 2 placebo-controlled studies, among the patients transferring directly from prior low-dose oral 5-aminosalicylic acid (approximately 50% in each treatment group), multimatrix 4.8 g/day was significantly more effective than placebo while the efficacy of multimatrix 2.4 g/day did not reach significance. In contrast, patients who had not received 5-aminosalicylic acid therapy for at least 5 days prior to receiving the study medication responded to both 2.4 g/day and 4.8 g/day.8 In the present study, the patients were allowed to use oral mesalazine up to a dose of 2.4 g/day during the screening period, and approximately 80% patients were directly transferred to each treatment group from their prior regimen (Table 1). Therefore, the dose-response relationship for the 2 doses (2.4 g/day and 4.8 g/day) of multimatrix mesalazine observed in the present study agrees with the results of the pooled subgroup analysis in the 2 previous placebo-controlled studies.
In the previous study of pH-dependent release controlled mesalamine (ASCEND I, ASCEND II, and ASCEND III), a higher dose of mesalamine (4.8 g/day) was observed to be of benefit in moderately active UC.9
10
11 In the present study, the change in UC-DAI in the Multimatrix-4.8 group was greater than in the other low-dose treatment groups not only in moderately active UC (UC-DAI score at baseline: 6–10) but also in almost all subgroups, including disease type (first attack, relapsing), disease region (proctitis, left-sided colitis, pancolitis) and mildly active (UC-DAI score at baseline: 4–5) with no associated safety concerns. This suggests that, in general, multimatrix 4.8 g/day is preferable to multimatrix 2.4 g/day for induction treatment in various disease states of mildly to moderately active UC.
In conclusion, the present study showed comparable efficacy between multimatrix mesalazine 2.4 g/day and controlled release mesalazine 2.25 g/day, although non-inferiority was not demonstrated. However, this was the first study to show that multimatrix mesalazine 4.8 g/day is more effective than 2.4 g/day. Moreover, this study also showed that the clinical benefit of multimatrix mesalazine 4.8 g/day in various disease conditions in mildly to moderately active UC with no associated concerns about safety.
 XML Download
XML Download