

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The burden of IBD in India and other Asian countries has increased in recent times, and the projected IBD population in India is second highest in the world after the United States.123 UC has a relapsing and remitting course, and acute severe colitis (ASC) complicates the course of UC in up to 25% of cases, with a third of these episodes being the first presentation of UC.45 The course of UC is similar between the West and Asia, and in an earlier prospective study, we found similar short-term colectomy rates and response to in-travenous (IV) steroids in 49 episodes of ASC.6 Truelove and Witts criteria7 are most widely used to define ASC.891011 The definition is based on 6 or more blood stained stools daily, with 1 or more of the 4 additional criteria: hemoglobin <105g/L, ESR >30 mm/h, fever >37.8℃, and tachycardia >90/min. Hemoglobin is 1 of the 4 relative criteria for the diagnosis of ASC. Nevertheless, the hemoglobin cutoff of 105 g/L is based on the normal levels of 130 g/L in men and 120 g/L in nonpregnant women, in the Western countires.12 In developing countries, the average hemoglobin in the population is lower, with normal being considered as 125 g/L in men and 110 g/L in nonpregnant women (Vietnam National Institute of Health study13) or 123 g/L and 110 g/L respectively, in a study from India.14 A lower hemoglobin in our country could lead to over-diagnosis of ASC if conventional Truelove and Witts criteria are applied, with needless hospitalization and increased cost or unnecessary IV corticosteroids.
This study was therefore planned to evaluate the relevance of Truelove and Witts criteria for diagnosing ASC in India.
METHODS
We diagnosed ASC using the conventional Truelove and Witts criteria and then assessed the effect on the rate of diagnosis of ASC, by excluding patients in whom the only positive additional criterion was hemoglobin <105 g/L. All consecutive patients diagnosed with ASC based on Truelove and Witts criteria who were hospitalized at All India Institute of Medical Sciences (AIIMS), New Delhi, India from April 2015 to December 2016 were screened for inclusion. Written informed consent was obtained from all patients. Children <18 years and patients refusing to give consent were excluded (ethical approval AIIMS IRB number: IESC/T-277).
1. Definitions
UC: diagnosis based on clinical, radiological, and histological criteria.15 Patients with first presentation of disease with ASC who were later found to be suffering from an infection or Crohn's colitis were excluded.
ASC: based on Truelove and Witts criteria; 6 or more stools with blood and 1 or more of hemoglobin <105 g/L, ESR >30 mm/h, fever >37.8℃, or tachycardia >90/min.78
Disease extent: maximum macroscopic extent on colonoscopy preceding ASC, according to the Montreal classification.16 For patients presenting with ASC at diagnosis, the extent was determined using the first colonoscopy after discharge or the surgical specimen if they underwent colectomy.
Prior steroid use: any use of systemic corticosteroids prior to the index episode of ASC. Steroid use in the first year of diagnosis: corticosteroids usage in the first year after diagnosis, including the ASC event if it occurred within the first year of diagnosis.
Ulcerative colitis endoscopic index of severity (UCEIS):17 the sum of 3 descriptors: vascular pattern (score, 0–2); bleeding (score, 0–3); and erosions and ulcers (score, 0–3), range from 0 to 8, assessed in the most severely affected area on flexible sigmoidoscopy (S.J.).
2. Study Design
This was a prospective, observational cohort study. Data on baseline demographics, prior therapy for UC, plain abdominal radiograph and endoscopic assessment of severity (UCEIS)17 using unprepared flexible sigmoidoscopy within 24 hours of admission, clinical observations of pulse rate, temperature, blood pressure, stool frequency, and laboratory parameters during the hospital stay were included. Serum CRP was performed on day 3 of IV corticosteroid therapy and Clostridium difficile toxin assay was performed using ELISA, for both toxins A and B. Subsequently the patients diagnosed with ASC were reclassified after excluding hemoglobin as one of the diagnostic criteria, to evaluate the confounding effect of baseline hemoglobin on ASC diagnosis.
3. Management
All patients received IV and rectal hydrocortisone (400 mg/day IV, 200 mg/day per rectum), whilst continuing 5-aminosalicylic acid therapy, according to the guidelines,18 as well as antibiotics (ciprofloxacin and metronidazole), given the prevalence of gastrointestinal infection in India. Blood transfusion was given as required (hemoglobin <80 g/L), mucosal biopsies were taken during flexible sigmoidoscopy to exclude cytomegalovirus (CMV) infection. Oxford criteria 19 were used to identify patients at high risk of colectomy and if unresponsive to 5 to 7 days of IV corticosteroids, rescue therapy or colectomy was advised. The choice, decision, and timing of colectomy was arrived at after a joint medical-surgical review and patient counselling. Patients responding to IV corticosteroids were discharged on 40 mg/day prednisolone with a tapering period of 3 to 4 months, along with azathioprine.
4. Statistical Analysis
Continuous variables were expressed as the mean±SD and those with non-Gaussian distribution as median and range. Categorical variables were summarized as frequencies with percentages rounded up or down to the nearest integer. Analyses were performed using SPSS software version 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
1. Patients
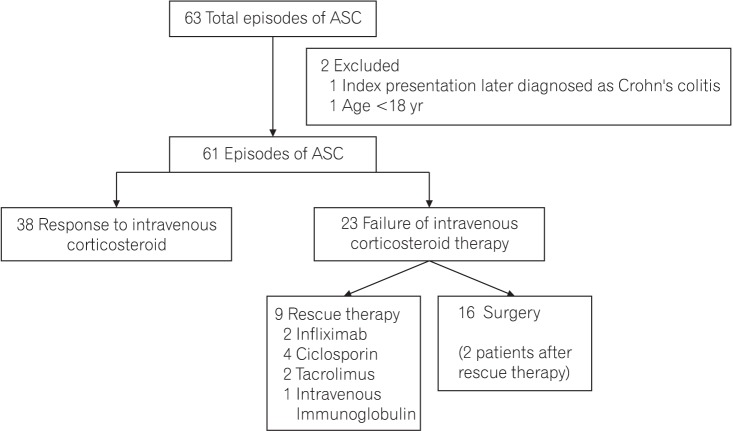
In all, 59 patients with 63 episodes of ASC were hospitalized during the study period, of which 2 patients were excluded (Fig. 1). Thus, 57 patients with 61 episodes of ASC were included in the study. Response to IV corticosteroids was seen in 38 of 61 episodes and 23 of 61 did not respond. Of these, 9 of 23 received rescue therapy (4 ciclosporin, 2 tacrolimus, 2 infliximab, and 1 patient received IV Immunoglobulin).2021 Sixteen of 23 patients underwent surgery, including 2 after rescue therapy.
2. Baseline Demographic and Clinical Characteristics
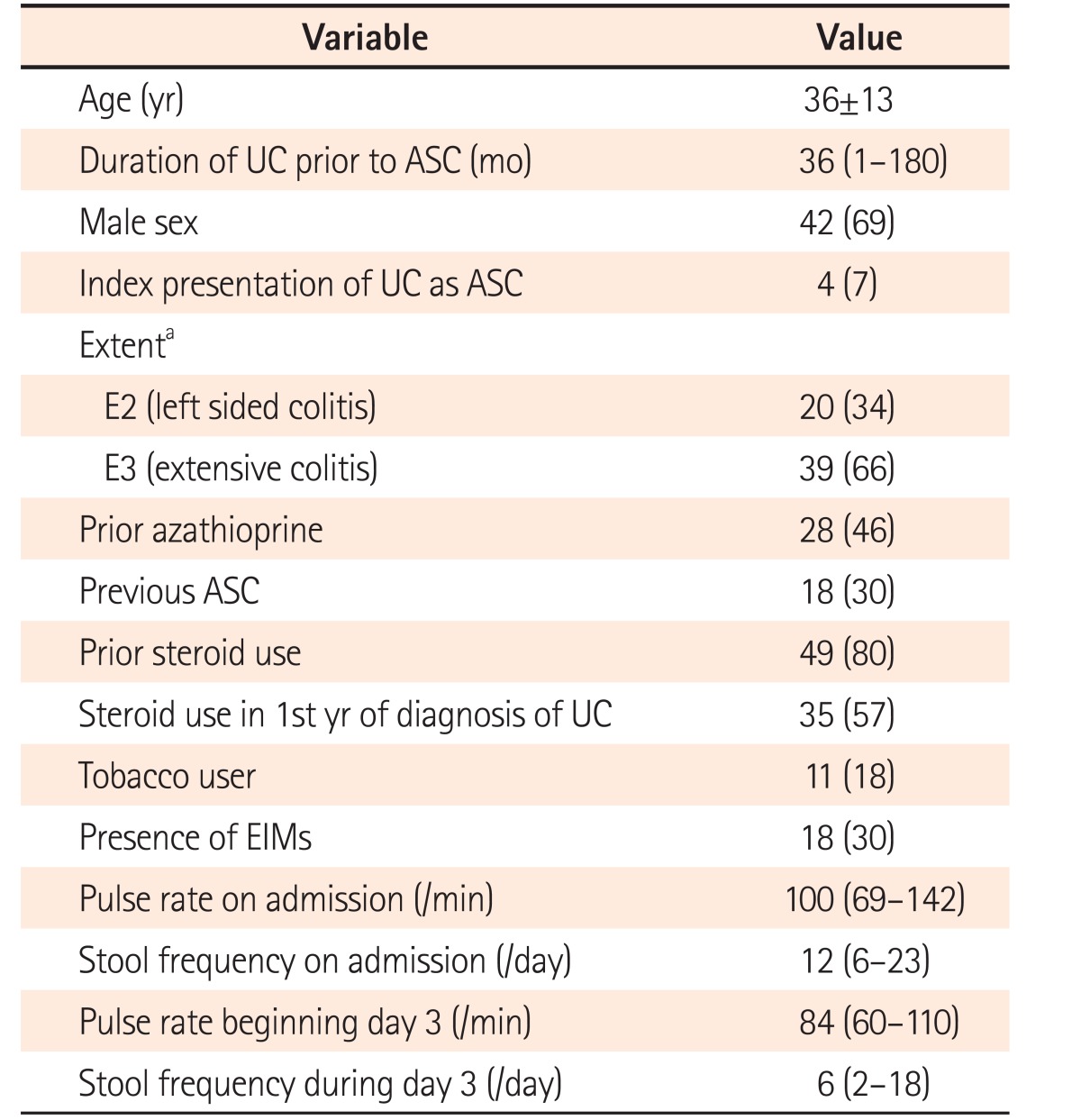
Mean age on admission was 36±13 years, 69% were men. Median duration of UC prior to diagnosis was 36 months and 7% presented with ASC at diagnosis. Two-thirds had extensive colitis and one-third had extraintestinal manifestations. One-third had history of a previous episode of ASC and 57% had used steroids in the first year of diagnosis, whereas 80% had used steroids at some stage after diagnosis (Table 1).
3. Clinical and Laboratory Parameters during Hospitalization
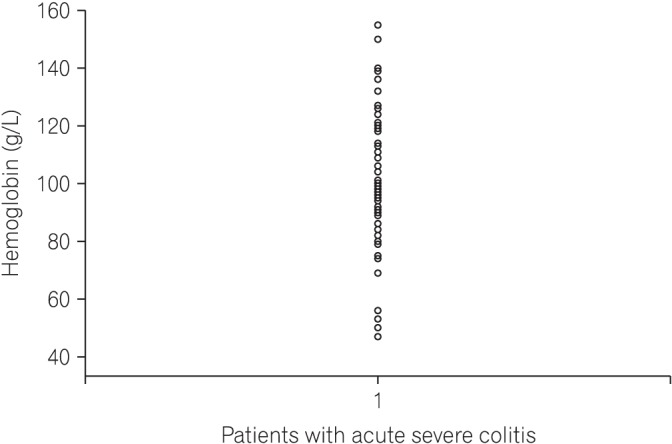
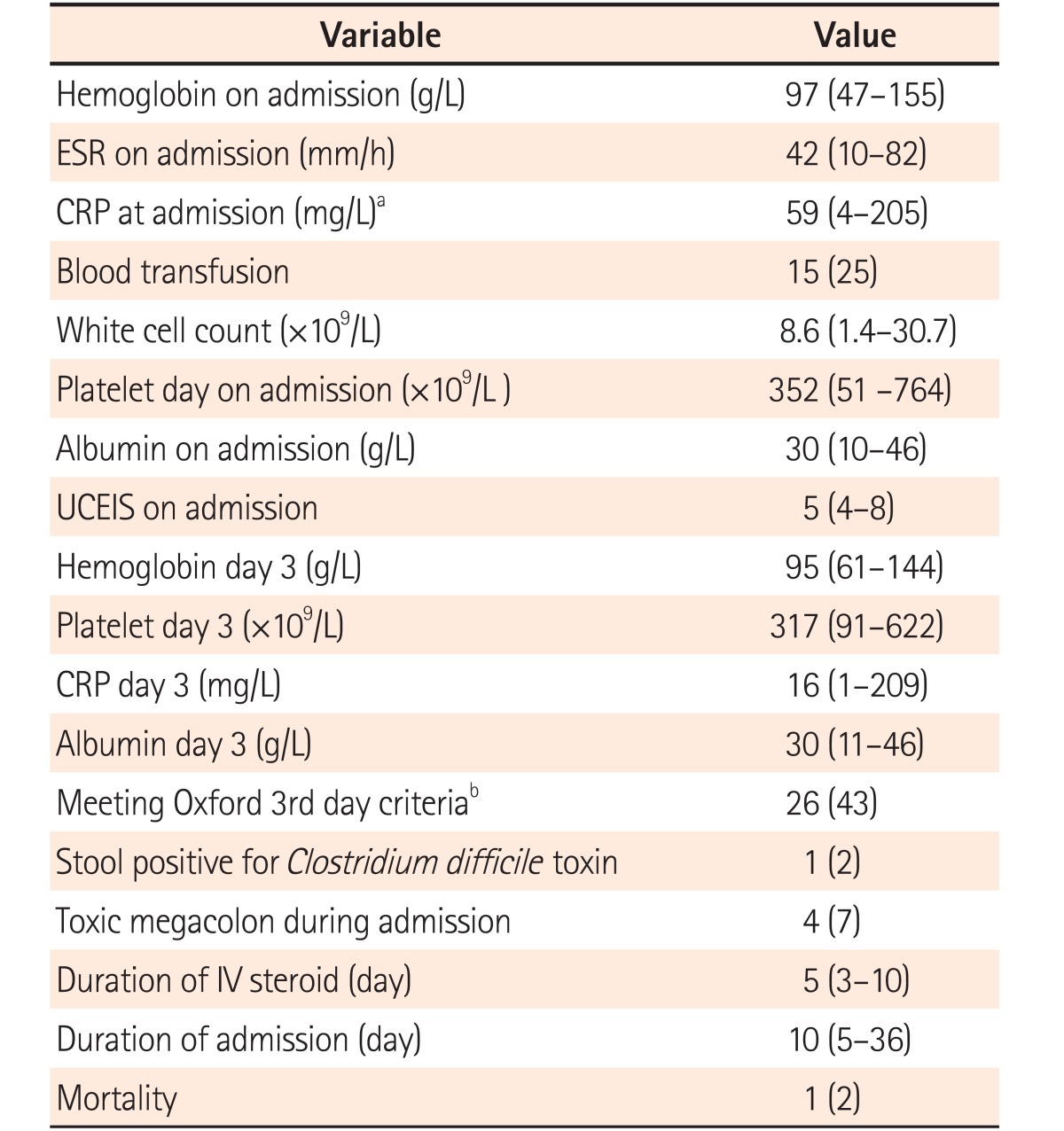
Median stool frequency on the day of presentation was 12 (range, 6–23), which decreased to 6 (range, 2–18) on day 3 of IV corticosteroids (Table 1). Median hemoglobin was 97 g/L (range, 47–155 g/L), ESR on admission was 42 mm/h (range, 10–82 mm/h) and 25% received blood transfusion(s) (Table 2, Fig. 2). Median CRP on day 1 was 59 mg/L (range, 4–205 mg/L). Median UCEIS was 5 (range, 4–8) and median CRP level on day 3 of IV corticosteroid was 16 mg/L (range, 1–209 mg/L). One patient was positive for C. difficile toxin in stool and cytomegalovirus immunohistochemistry was positive in 10 of 61 episodes (16%). Patients received IV corticosteroids for a median 5 days (range, 3–10 days) with the duration of hospital stay being 10 days (range, 5–36 days). Four patients developed toxic megacolon, all of whom underwent colectomy. One patient died on postoperative day 3 from ventricular arrhythmia because of hypokalemia.
4. Truelove and Witts Criteria at Admission
1) All Criteria
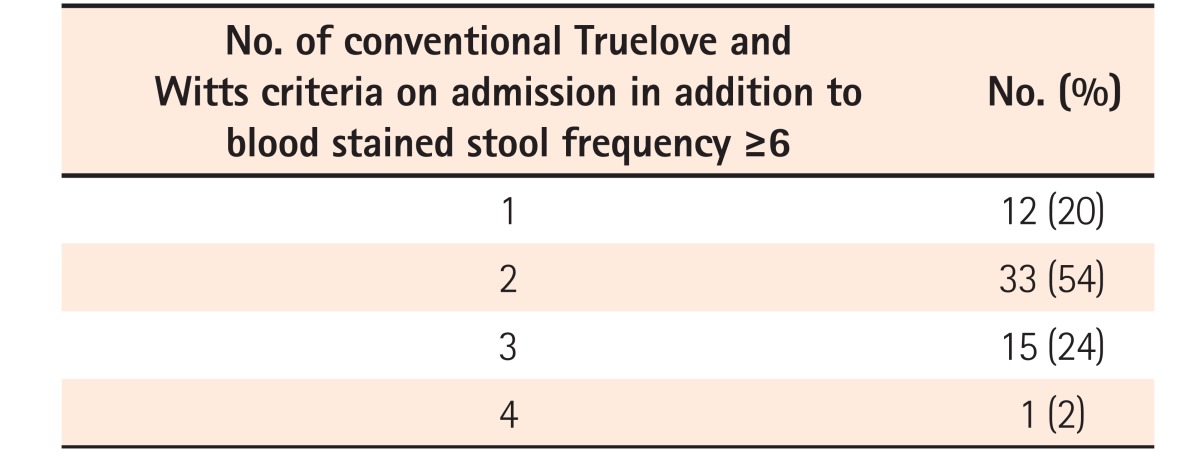
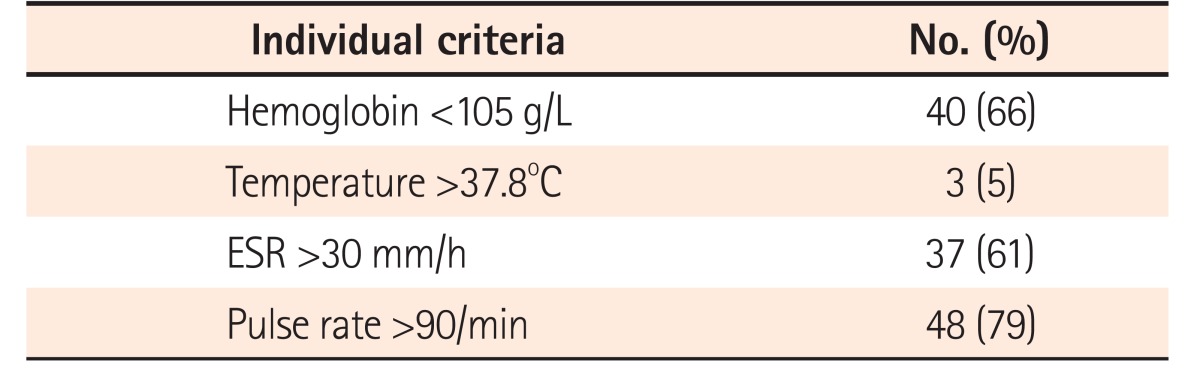
All patients had ≥6 blood stained stools/day at admission. Twelve patients (20%) had 1 additional criterion, 33 (54%) had 2 additional criteria, and 16 (26%) had 3 or more additional criteria on admission (Table 3). The most common additional criterion was tachycardia (pulse rate >90/min) seen in 48 of 61 episodes (79%), followed by hemoglobin <105 g/L in 40 (66%), ESR >30 mm/h in 37 (61%), whereas fever was least common, seen in only 3 of episodes (5%) (Table 4). CRP on admission >30 mg/L was seen in 39 episodes (64%). Among patients who had only 1 additional criterion (n=12) the most common criterion was tachycardia (n=10), followed by ESR >30 mm/h (n=2). None of the patients had hemoglobin as the only additional criterion.
2) Excluding Hemoglobin
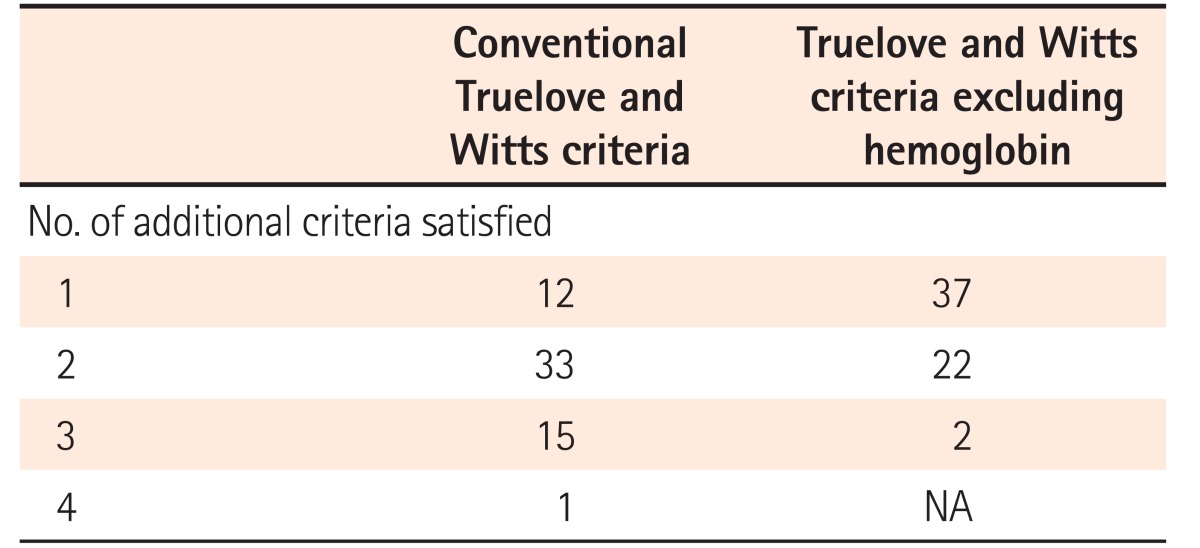
On excluding hemoglobin as an additional criterion, all patients still classified as ASC, but now with 37 of 61 (61%) having only 1 additional criterion and 24 (39%) having 2 or 3 additional criteria on admission (Table 5).
DISCUSSION
In this prospective cohort study of 61 consecutive episodes of ASC in 59 patients, we found that 80% of the episodes were associated with 2 or more additional Truelove and Witts criteria on admission, of which the commonest were tachycardia and low hemoglobin. The median hemoglobin on admission was 97 g/L (range, 47–155 g/L), which is lower than that seen in Western studies.192223 However, only 20% of the episodes were associated with a single additional Truelove and Witts criterion, of which none had hemoglobin <105 g/L as the only additional criterion. This was lower than the rate of 40% reported in previous studies.424 Even among Indian women, who have lower mean hemoglobin levels, with minimum population thresholds reported as 113, 110, and 100 g/L in studies by Ashavaid et al.,14 NIN criteria13 and Pasupula and Reddy,25 none of the episodes had hemoglobin as the only additional criterion for diagnosis of ASC. Therefore, after excluding hemoglobin as an additional criterion based on the original Truelove and Witts definition, all episodes still classified as ASC. Conceptually, ASC presents when the inflammatory activity of UC causes systemic manifestations of inflammation. This may explain why there appears to be no confounding effect of excluding hemoglobin on the diagnosis of ASC, despite a lower mean hemoglobin in the Indian population. It needs to be mentioned that Truelove and Witts criteria have never been subject to a mathematical analysis of the contribution of components to the diagnostic value of the index, which would be standard practice in the development of indices today.26 Patients with ASC have other signs of systemic inflammation that are manifest along with low hemoglobin, thereby maintaining the relevance of Truelove and Witts criteria other than hemoglobin, in this setting.
Both ESR and pulse rate increase with anemia, and this may further question the validity of Truelove and Witts criteria in the Indian setting, with an elevated ESR or tachycardia being a feature of anemia rather than systemic inflammation. However, patients identified with ASC in the present study had a short-term colectomy rate of 26% and steroid failure rate of 38%, which are very similar to reports from the West.4 Using CRP >30 mg/L instead of an ESR >30 mm/h would have strengthened our conclusions, since CRP is independent of anemia, and 39 of 61 patients (64%) had CRP >30 mg/L on admission. Although 8 of 39 patients with an elevated CRP had normal ESR, all had at least 1 other Truelove and Witts criterion for the diagnosis of ASC.
The limitations of this study include referral bias owing to the tertiary nature of our institution and the lack of data about outpatients with an acute flare up of colitis and hemoglobin <105 g/L. According to the protocol at AIIMS, patients with blood stained stool frequency >6/day and hemoglobin <105 g/L merit admission, but it cannot be confirmed that clinicians did not make an allowance for lower hemoglobin in the Indian population and treated them as outpatients. Whilst this may explain the absence of any patient with a low hemoglobin as the only additional criterion, it also indicates that they can be managed as outpatients. These results also need validation in other centers.
We conclude that Truelove and Witts criteria are relevant in the Indian settings, which is reassuring given the lower mean hemoglobin in the general population.
 XML Download
XML Download