

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The emergence of biologics has revolutionized the management of IBDs. Despite the accumulated clinical experiences of biologics usage, ongoing controversies still exist regarding the time for discontinuation. Additionally, their level of effectiveness when used for the second time also remains mostly unknown. Even at this time, recommendations of when to stop anti-tumor necrosis factor (anti-TNF) therapy cannot be made because of insufficient data.1 Cessation of biologic therapy can be due to various reasons, including cost and concerns about long-term safety.2 Recently, a European expert panel proposed that the withdrawal of anti-TNF therapy in CD patients may be appropriate after 2 years of clinical and endoscopic remission, and after 4 years of clinical remission.3
In Taiwan, adalimumab (ADA) is the only reimbursed biologic available for moderate to severe CD patients with a CDAI of more than 250 in cases in which other treatments have failed or following the discovery of adverse effects after use of conventional therapy for 6 months.4 Due to budget limitations, however, the National Health Insurance only allows for a limited period (i.e., approximately around 1 year) of biologics use in CD patients. In certain cases, once the biologic is discontinued, it can be temporarily reapplied following clinical relapse, or, if approved, restarted as a continued treatment.4
The criteria in Taiwan for starting treatment of biologics for CD is more stringent than in most other cases (the CDAI score is more than 250 for Taiwan, and 220 for most of the other studies reported); furthermore, most of the treatment policies for biologics use in Western countries and in Japan and Korea is lifelong use when necessary, while in Taiwan, the use is for a limited period. Therefore, using this study as an investigational tool, we would like to know whether the relapse rate was higher or the same after discontinuing the biologics and how effective biologics are when used as a 2nd treatment in CD patients, as well as whether there is any possible adverse events that may occur when used as the second treatment. Since ADA is an antibody, use for the 2nd time might result in problems including the increased development of anti-drug antibodies, as well as anaphylaxis. Therefore, we conducted this study with the aim to reveal the remission duration, the risk factors of relapse after discontinuing ADA, and the response and possible adverse effects of the second use of biologics.
METHODS
A multicenter retrospective clinical study was conducted involving 8 tertiary referral centers in Taiwan. For the purpose of this study, the CD diagnosis was based on established clinical, endoscopic and histological criteria.5 One hundred and twenty-three patients with active CD, who had received the loading dose as 160 mg, 80 mg and then followed by 40 mg every 2 weeks as maintenance therapy after conventional therapy failed to control the disease activity, were included in this study. This study was waived for informed consent.
Data detailing patient demographics including sex, smoking habits, previous surgical status, age at the time diagnosis, time of initiation and withdrawal from ADA, and use of concomitant medication was collected. Information collected regarded withdrawal included: the reason for withdrawal, Montreal classification and behavior, clinical remission or response and CDAI. Statistics on hemoglobin, white blood cell count, platelet, CRP levels and, when available, fecal calprotectin (fC), were collected within 1 month of the last ADA injection. Subsequent analysis focused on the patients who had attained a state of clinical remission, proportion, and time to relapse. The CADI was evaluated every 6 months, both before and after ADA treatment. Colonoscopy was performed as and when needed clinically, but not routinely.
1. Outcomes and Definition
The clinical remission was defined as CDAI <150 points, while clinical response was defined as a decrease in CDAI score of ≥70 points after using ADA. In all patient participants, anti-TNF therapy was discontinued, either due to clinical remission, or without clinical remission, but with National Health Insurance disapproval. Patients were then followed up every 2 to 12 weeks at the outpatient clinic. Relapse was defined as an increase in CDAI score of ≥70 points, or a CDAI score of more than 250. Deep remission was defined as clinical remission and complete mucosal healing. The indication for restarting ADA was a clinical relapse, together with insurance approval.
The primary outcome of this study was proportion of relapse and time to relapse after withdrawal of ADA, and then the identification of factors associated with the risk of relapse. The secondary outcome was tolerance, safety, and efficacy of retreatment with ADA in CD patients.
2. Statistical Analysis
Descriptive statistics for continuous variables were calculated and reported as mean±SD. The categorical variables were described using frequency distributions, and were reported as number (%). P -values were based on a 2 sample t-test for continuous variables and either chi-square or Fisher exact test was used for the categorical variables. Risk factors related to time to relapse was studied by multivariable proportional hazard analysis. Sensitivity and specificity were estimated with a receiver operating characteristic (ROC) curve analysis. The areas under the ROC curve (AUCs) were calculated for laboratory parameters of fC, CRP levels, hemoglobin, leukocyte, and platelets. The cutoff values were selected by the Youden index, using ROC curves. Statistical analysis was performed using the SPSS for Windows version 12.0 (SPSS Inc., Chicago, IL, USA). Tests were 2-tailed with a significance level of 0.05.
RESULTS
1. Baseline Characteristics
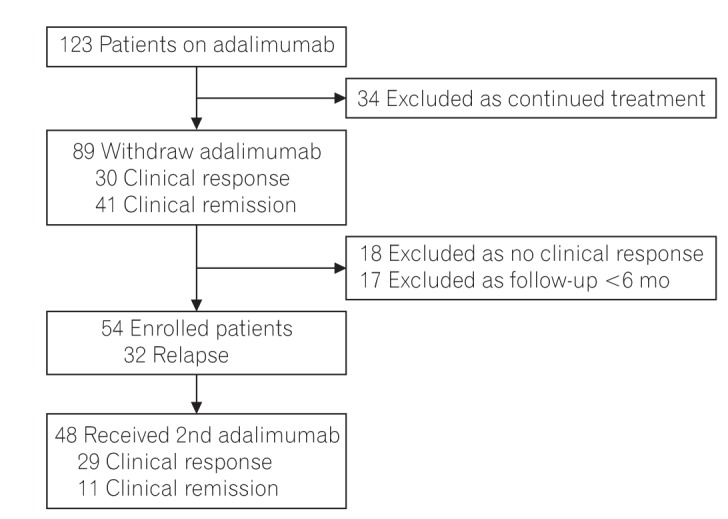
A total of 123 patients with moderate to severe active CD had used ADA between September 2009 and March 2016. Apart from the 34 patients who were continuously treated by way of self-finance, 89 patients had discontinued ADA after a limited period of treatment. At the time of discontinuing ADA, 30 patients achieved clinical response and 41 patients achieved clinical remission. Eighteen patients with no clinical response to ADA treatment, and 17 patients with a follow-up period of less than 6 months were excluded for the following analysis. A total of 54 patients had been followed up for more than 6 months after withdrawing of ADA were enrolled in this study. Among them, 32 patients (59.3%) suffered from clinical relapse after treatment cessation. The flowchart of patients is shown in Fig. 1.
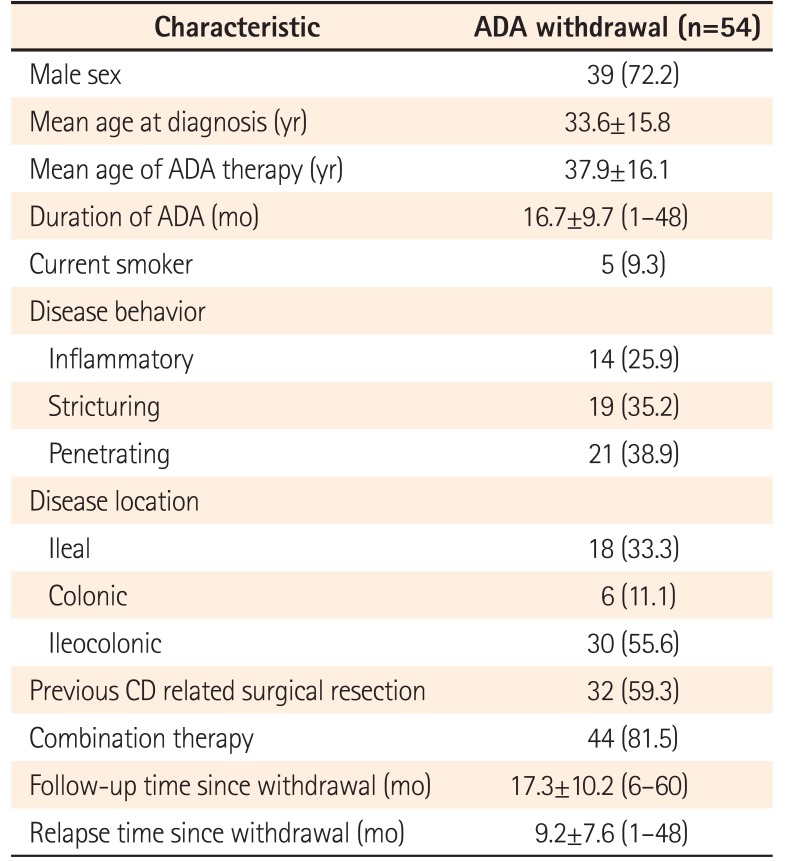
Among the 54 CD patients, 72.2% were male, and the mean age at diagnosis was 33.6±15.8 years (Table 1). The mean age of using ADA was 37.9±16.1 years old. The follow-up time since withdraw was 17.3±10.2 months, and relapse time was 9.2±7.6 months. Thirty-two patients (59.3%) had received surgery for CD, and 5 patients (9.3%) were smokers. With regards to disease behavior at diagnosis, the penetrating type of CD was the most common (38.9%), followed by the stricture type (35.2%) and then the inflammatory type (25.9%).
2. Reason of Withdrawal of ADA and Risk Factors for Relapse
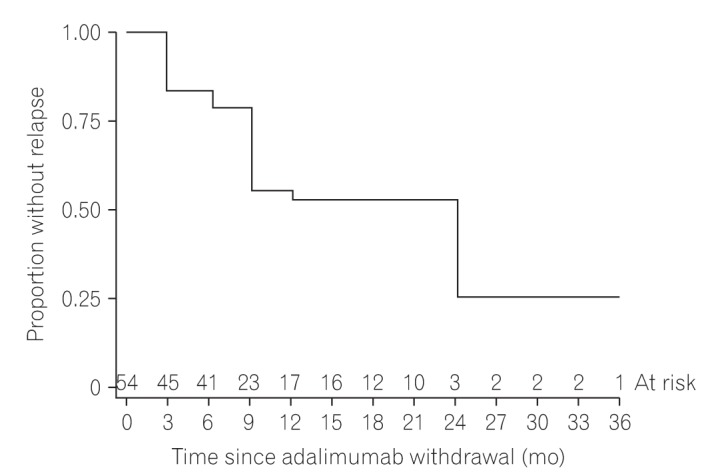
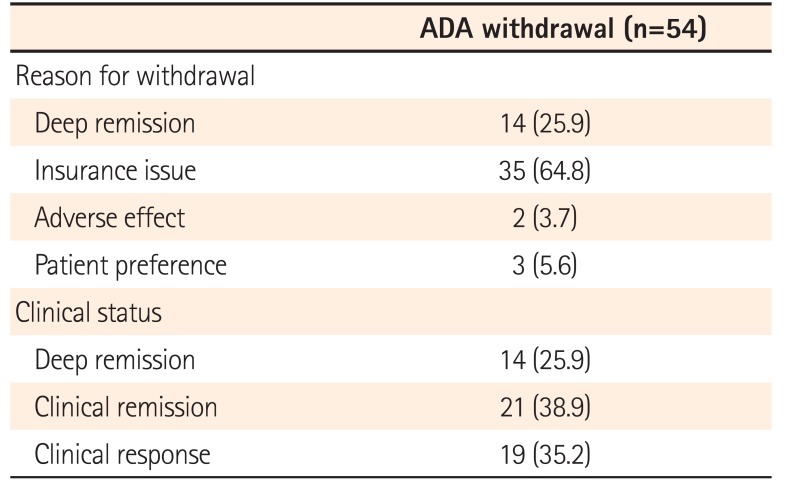
As for the reason of withdrawal from use of ADA, 35 patients (64.8%) stopped the treatment due to reimbursement issues; 14 patients (25.9%) achieved deep remission; 2 patients (3.7%) experienced adverse effects and 3 patients (5.6%) stopped the medication due to patient preferences (Table 2). At the timing of withdrawing ADA, 21 patients (38.9%) achieved clinical remission; 19 patients (35.2%) achieved clinical response; and 14 patients (25.9%) had deep remission. Thirty-two patients suffered from relapse after withdrawing from the use of ADA, and the time-to relapse curve is shown in Fig. 2. The relapse rates at 12 and 24 months were 43.4% and 75%, respectively, with a median time to relapse of 14 months.
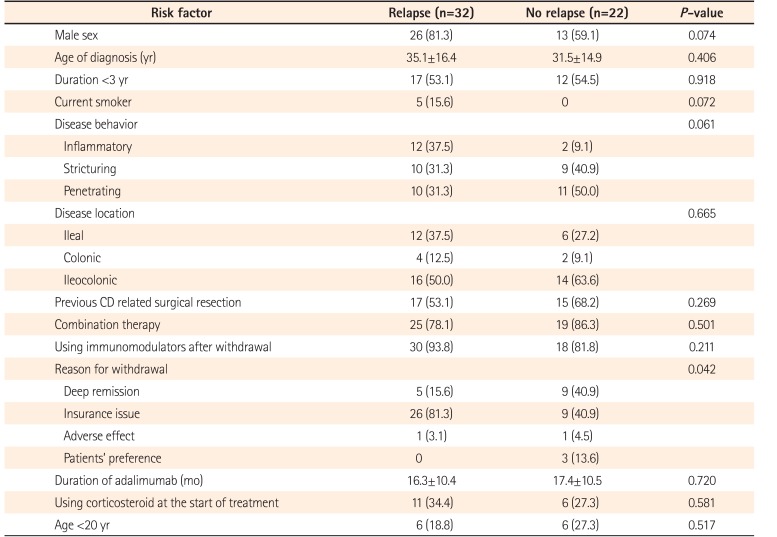
As for the predictive factors for relapse in these 54 patients, there was no statistical significance in age, sex, disease duration, disease location and behavior, smoking history, operation for CD and/or combination of treatments (Table 3). Study results indicated that the longer mean time of using ADA decreased the relapse rate, but without statistical significance (17.4 months vs. 16.3 months, P =0.462). Reasons for ADA withdrawal were the significant factors for predicting the relapse (P =0.042) of CD. These factors included non-medical reasons related to insurance reimbursement (81.3% patients with clinical relapse vs. 40.9% patients with no clinical relapse, P =0.002) and medical reasons related to deep remission (15.6% patients with clinical relapse vs. 40.9% patients with no clinical relapse, P =0.037) for ADA withdrawal.
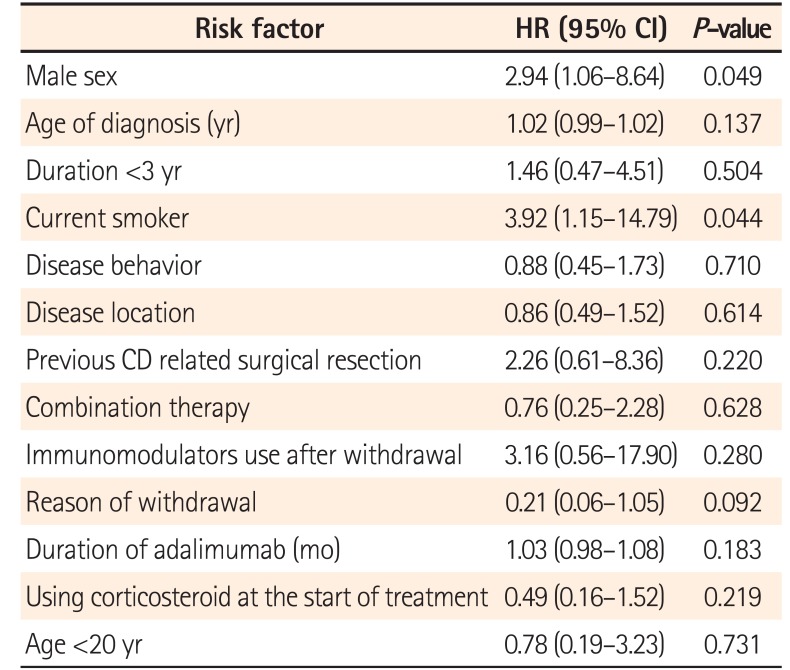
Variables associated with time to relapse in multivariable analysis were presented in Table 4. Current smoker became an important risk factor of relapse (OR, 3.9; 95% CI, 1.2−14.8; P =0.044). Male sex was another risk factor of relapse (OR, 2.9; 95% CI, 1.1−8.6; P =0.049). There was no statistical difference regarding the reason of withdrawal in the multivariable analysis.
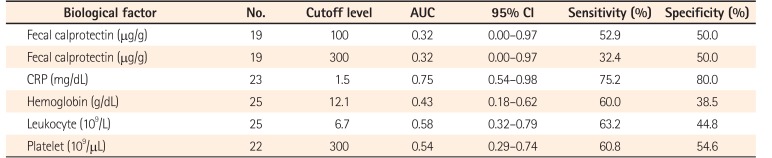
With regards to the laboratory parameters which were checked within 1 month after withdrawal from ADA, the best discriminative cutoff was obtained at a CRP with the threshold of 1.5 mg/dL, which could predict clinical relapse with 75.2% sensitivity and 80.0% specificity (AUC of 0.75) (Table 5). The threshold of 2 another parameters for a higher risk of relapse are as follows: leukocyte ≥6.7×109/L, and platelet ≥300×109/L, with AUC 0.58 and 0.54, respectively. Due to the small sample size, fC in this study did not show any predicting power of relapse.
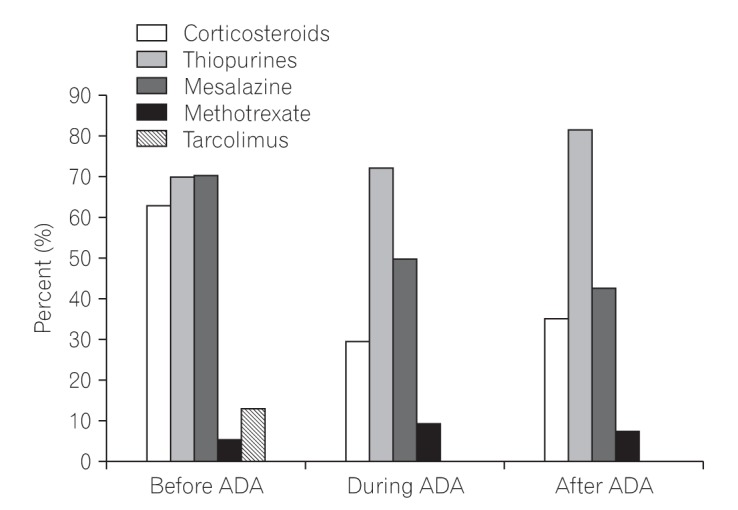
The medications used before, during and after ADA treatment are listed in Fig. 3. Seventy-nine percent of patients (43 of 54) were treated with immunomodulators before initiation of ADA treatment. Concomitant immunosuppression during ADA usage was observed with thiopurines in 72.2%, and with methotrexate in 9.3% of the patients. There was no statistical difference in use of combination treatments with regards to relapse (78.1% vs. 86.3%, P =0.444). Interestingly, the immunosuppression agents were used more frequently in the relapse group after withdrawal of ADA, but also without statistical significance (93.8% vs. 81.8%, P =0.170).
Thirty-three patients with clinical relapse and 15 patients with a surgery history for CD received the second round of biologics. Among these 48 patients who received second treatment, a clinical response was seen in 29 (60.4%) and clinical remission was seen in 11 (22.9%), upon evaluation at 3 months after the re-treatment. The observed period of secondary treatment with ADA was 6.8±4.5 months. After re-initiation of ADA therapy, 1 patient suffered from anaphylaxis.
DISCUSSION
The use of drugs anti-TNF has greatly improved the therapeutic outcome, leading to fewer hospitalizations and surgical procedures.6 In Asia, most physicians prefer to first use thiopurine, followed by anti-TNF therapies in steroid-refractory CD.7 CD is a chronic relapsing-remitting disease, and patients are expected to relapse eventually in long-term sustained remission after discontinuing anti-TNF therapy.8 Despite heterogeneous study designs and patient populations, a systemic review study found thatand 2-year relapse rates ranged from 21.1% to 39.0% and from 37.0% to 55.7%, respectively, after anti-TNF withdrawal from clinical remission.9 Rismo et al.10 reported higher rates of relapse (52% at 6 months and 74% at 12 months), which potentially relate to short treatment duration before withdrawal. Our results also demonstrated that relapse rate was 24.1% at 6 months and 43.4% at 12 months, respectively, after a mean of 16.7±9.7 months of ADA treatment.
In the present retrospective study, we examined the predictors of clinical relapse in ADA-treated CD patients. Male sex and current smoker after ADA withdrawal were identified as predictors of the need for resumption of biological therapy. The STORI trial revealed male sex, leucocyte count >6.0×109/L, hemoglobin ≤14.5 g/L, a CRP level ≥5.0 mg/L, and fC ≥300 µg/g as predictors of relapse after the cessation of biological therapy.11 Another study also showed that sex and BMI were independently influenced the pharmacokinetics of infliximab, and that high BMI and males had higher clearance of TNF antagonists.12 Furthermore, additional research involving 3,420 registry patients in the infliximab-treated group showed that being of the female sex had a protective effect (hazard ratio, 0.71; 95% CI, 0.53−0.96; P =0.023).13
Current smoking played an important role in the risk of relapse of CD.14 In patients who received operation for CD, smoking increased 2-fold risk of recurrence compared with non-smokers.15 In the biologic era, the first study to prospectively assess the effect of smoking cessation on CD relapse showed continuing smokers had earlier relapse even they had been prescribed anti-TNF.16 Patients who continued to smoke had a greater incidence of relapse compared to non-smokers (hazard ratio, 1.53; 95% CI, 1.10−2.17), and non-smokers had similar relapse rates to those who had quit and to those who were former smokers.16 Therefore, encouraging patients to stop smoking is an important part of the management of CD.
Previous study has also shown that patients with shorter disease duration have a better response to early treatment.17 However, there is no significant difference in clinical remission and relapse with shorter disease duration (<3 years).17 Our study also revealed the same result; namely, that there is no significant difference when using ADA in the short disease duration of less than 1.5 years.
The relapse rates at 12 and 24 months after the discontinuation of biological therapy was higher in our study (43.4%−75.0%) than in the STORI study (43.9%−52.2%).11 This discrepancy might be because the median duration of biologic agent therapy was more than 2 years in the STORI trial, whereas it was only more than 1 year in our study. Most patients relapse after stopping anti-TNF therapy if followed long enough. An observational retrospective study revealed 53 patients with CD stopped infliximab while in clinical remission and were monitored for up to 10 years; after stopping infliximab, the percentage of CD in remission dropped from 50% to 12%, respectively, at 2 and 10 years.18
CRP is one of the most frequently studied laboratory parameters when predicting disease course in IBD. Patients with a high CRP have a higher chance of achieving and maintaining a response to biological therapy than do patients with a low or normal CRP.1 However, the presence of systemic inflammation increases protein catabolism in the reticuloendothelial system, and an increased serum concentration of CRP has been associated with increased drug clearance.19 The present study revealed that a CRP level ≥1.5 mg/dL, checked at the withdrawal of biological therapy, was associated with a higher probability and shorter duration of time necessary to reinitiate biological therapy. However, since the number of patients examined in this study was small that we cannot conclude it as a definite risk factor.
Previous studies have shown that an increased concentration of fC is a good predictor of clinical relapse in patients with UC, but most studies did not include patients with CD.2021 A study showed fC measurement at entry or at week 14 cannot predict clinical relapse in patients in remission with Infliximab.22 However, other studies showed higher fC levels 2 months after first infusion of infliximab or fC level >50 mg/g at time of anti-TNF withdrawal could be the predictive factors for relapse.2324 We did not observe that fC could predict the relapse, probably due to small sample size.
It has been reported that retreatment with the same anti-TNF drug in CD patients who relapsed after discontinuation of anti-TNF therapy induced remission in 82% of patients.25 However, in our study, the clinical response rate was lower in the retreatment patients than the first treatment patients (60.4% vs. 79.8%). Anti-drug antibody could not be assessed, therefore, although we thought that the developing of anti-drug antibody might contribute to the lower response rate when as the 2nd use of anti-TNF antibody.
Noteworthy was the adverse effects when with the 2nd treatment. The most common reactions of ADA were mild injection site reactions in up to 20% of patients and fewer than 1% of patients experienced allergic rash or urticaria.26 Anaphylactic reactions wound not only occur in the initial treatment, but also a delayed-type hypersensitivity reaction could occur. One report showed a patient with anaphylactic shock following the 11th ADA.27 The re-exposure of infliximab after suspension of treatment have also been reported.28 In our patients, there was 1 patient who had anaphylaxis after re-exposure to ADA and 3 patients had adverse effect (dizziness and epigastria) in the initial second ADA treatment in this study.
The limitations of our study are its retrospective nature and the shorter follow-up after drug withdrawal; thus, the true efficacy and impact over long-term merits further evaluation. Our study was not steroid-free remission and nearly 29.6% patients used steroid during ADA prescription. fC was collected in fewer patients, because it was used in a study in Taiwan, and would affect clinical significance of relapse. The anti-ADA antibody and ADA concentrations were not obtained in this study, which also played a role in the clinical remission and relapse.
In conclusion, male sex and current smoker are risk factors of relapse after limited period of ADA treatment in Taiwanese CD patients. Cessation of biologic agents is associated with 43% risk of relapse 1 year after withdrawal of the biologics. Longer treatment with higher possibility of mucosal healing may benefit the patient.
 XML Download
XML Download