

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Inflammatory bowel disease (IBD) includes UC and CD, which are chronic idiopathic systemic diseases that involve chronic inflammation of the intestine. Although their etiopathogenesis remains an enigma, it is thought that they are complex polygenic disorders, involving interplay of environment, gut microbiota, and dysregulated immune activation in genetically predisposed individuals.12
Family history includes a combination of both genetic and environmental influences. A positive family history has been found to be a strong risk factor for the development of IBD, more so for CD than UC.34 Increased disease concordance among monozygotic and dizygotic twins points strongly towards the role of genetics in the development of UC.56 Although genome-wide association studies have identified several overlapping loci that are associated with both UC and CD,7 family history for UC is less well established as a risk factor than for CD, and more studies are required.
The burden of IBD in India and other Asian countries is rising.8910 Several studies from the West have determined the prevalence of IBD in the relatives of UC or CD patients. Data from Copenhagen report a 10-fold increase in the familial risk of UC.11 In a pediatric study in Greece that included 244 UC patients, 6.6% had a positive family history of UC.12 There are very few studies in the Asian population. The early course of disease in patients with IBD in Asia was found to be comparable to that in the West.13 However, the prevalence of an associated family history in the Asian population was found to be less than that in the Western population.1415
There are currently no available data from India on the prevalence of family history in patients with UC. Thus, we undertook this study, with a large sample size, to assess the prevalence of UC in the first- and second-degree relatives of Indian patients with UC, and to study the phenotype and long-term disease behavior in those with a positive family history. The study of the familial aggregation of UC may be crucial in better elucidating the genetic component of this disease.
METHODS
1. Study Population
Patients with UC followed at the Inflammatory Bowel Disease Clinic at the All India Institute of Medical Sciences (AIIMS), New Delhi, from August 2004 to January 2016 formed the background population of this study. AIIMS is a tertiary care center, serving as a referral hospital for patients from all over North India. Diagnosis of UC was established on the basis of accepted clinical, endoscopic, radiological, and histological criteria.16
2. Study Design and Data Collection
This study is a retrospective analysis of a referral IBD registry. Relevant clinical data were obtained from medical records encompassing both the initial consultation as well as subsequent follow-up through the entire duration of care within the practice. The medical records are comprised of a system of files, with each patient assigned an IBD number. Each file contains detailed information about the patient's disease and follow-up, including name, age, sex, phone number, address, diagnosis, history, clinical examination, investigations, and ongoing treatment. Approval was obtained from the ethics committee before starting the study.
We reviewed the medical records of UC patients who had a positive family history of IBD. These were used to assess the prevalence of UC in the first- and second-degree relatives of patients with UC. When ≥2 members of the same family were registered, the member in whom UC was first diagnosed was considered the proband, and the others were regarded as relatives. First-degree relatives comprised parents, children, or siblings; second-degree relatives included grandparent-grandchild, and aunt/uncle-niece/nephew. A positive family history was defined as a proband having at least one first- and second-degree relative with IBD.
Information was obtained on demography, age at onset of UC, age at diagnosis, duration of illness, extent, extraintestinal manifestations, surgery, number of first- and second-degree relatives affected, and their diagnosis. Similar details were also obtained for each affected first-degree relative. We further collected information from the patients and their relatives by telephonic interviews, and interviewed them in person during their visit. Approval was given by the Institutional Ethics Committee.
3. Statistical Analysis
Categorical variables were compared between groups using the chi-square test. Continuous variables with normal distribution, e.g., age at onset, were compared using Student t-test for independent samples. However, a nonparametric test for independent samples, i.e., the Mann-Whitney U test, was used for continuous variables that did not have a normal distribution. The Spearman rank correlation coefficient was used to compare continuous clinical characteristics in patients and their relatives. A P-value was considered significant when less than 0.05. Statistical analysis was performed using STATA for Windows version 14.1 (StataCorp., College Station, TX, USA).
RESULTS
1. Study Population
We included a total of 2,058 patients with UC in this study, of whom 65.4% were male. The mean age at onset of symptoms was 32.2±12.1 years, and at diagnosis was 32.5±12.1 years. The mean duration of illness was 5.8±6.7 years. The proportions of patients with proctitis, left-sided colitis, and extensive colitis were 14.8%, 42.3%, and 42.9%, respectively.
2. Prevalence of IBD in First- and Second-Degree Relatives
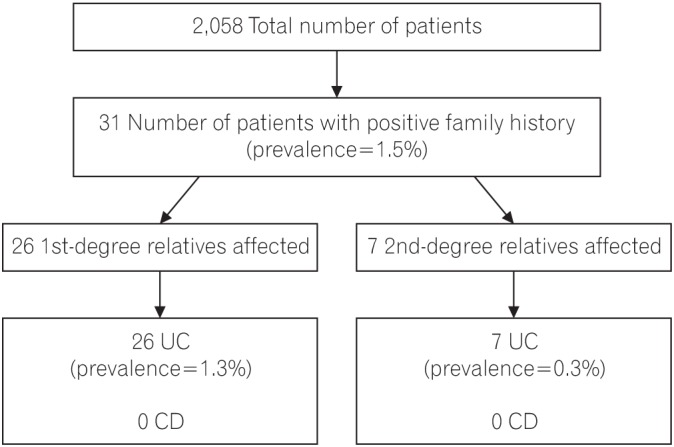
Of the 2,058 patients included in the analysis, a positive family history of IBD was confirmed in 31 patients (1.5%), (Fig. 1) 24 (77.4%) of whom had only first-degree relatives affected; 5 patients (16.1%) had only second-degree relatives affected and 2 patients (6.5%) had both first- and second-degree relatives affected. Hence, the prevalence of IBD among first-degree relatives was 1.26%, and among second-degree relatives, 0.34%. A total of 25 patients each had only 1 affected family member (80.7%), while 6 patients each had 2 affected family members (19.4%). All the affected relatives were diagnosed with UC; hence, the concordance for type of IBD was 100%.
3. Comparison of Clinical Features in Patients with Sporadic and Familial UC
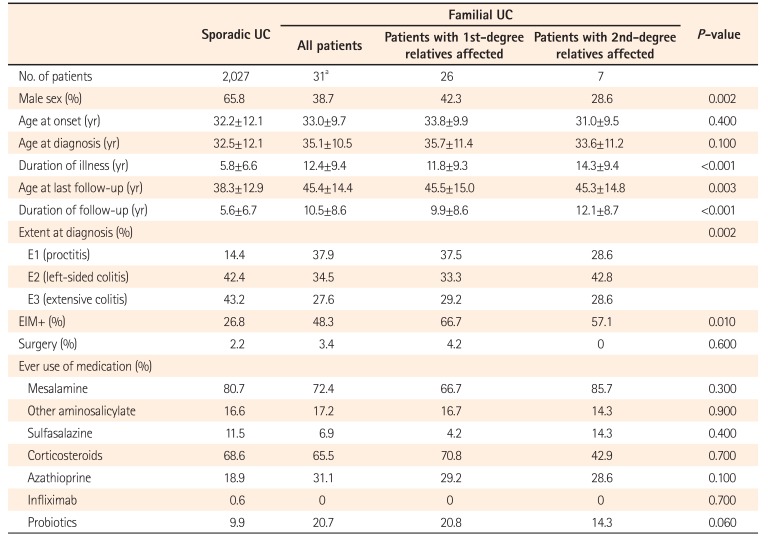
The proportion of male patients was significantly lower in familial cases (38.7%) than in sporadic cases (65.8%, P=0.002). There was no significant difference in mean age at onset (33.0±9.7 years vs. 32.2±12.1 years, P=0.400), and mean age at diagnosis (35.1±10.5 years vs. 32.5±12.1 years, P=0.100). The extent of disease also varied significantly, with E3 disease being less common in familial cases (27.6%) than in sporadic cases (43.2%, P=0.002). Most patients (79.3%) with familial UC had an intermittent flare type of disease course, whereas 13.8% and 6.9% had a chronic continuous type or a single episode of UC, respectively. Nearly half (48.3%) of the familial cases reported extraintestinal manifestation; the proportion was higher in patients with an affected first-degree relative (66.7%), while it was significantly lower in sporadic cases (26.8%, P=0.010). There were no significant differences in terms of surgery and the use of medications among the patients with and without a family history of UC (Table 1).
4. First- and Second-Degree Relatives with UC: Clinical Characteristics
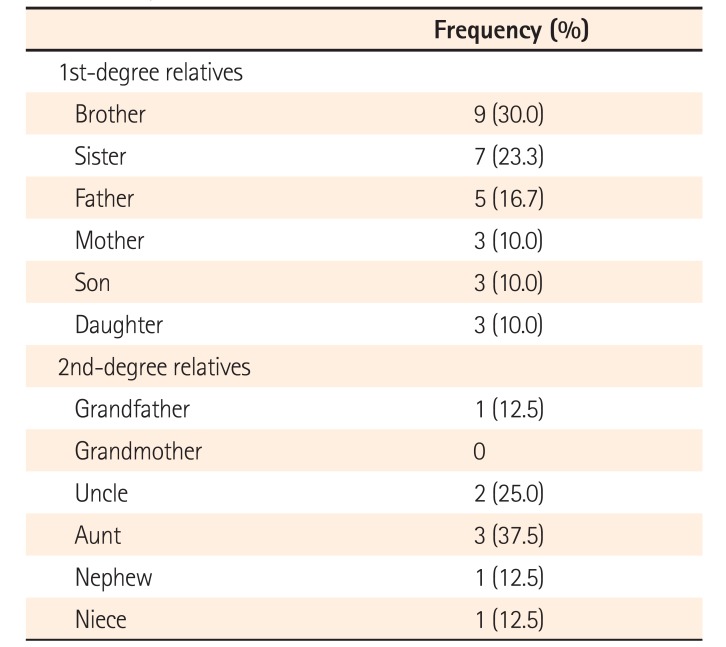
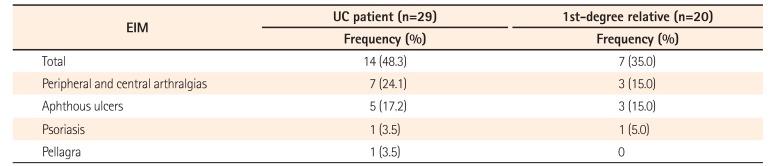
The frequency of IBD among first- and second-degree relatives of patients with UC according to type of relationship is shown in Table 2. Among first-degree relatives, siblings were found to have the highest prevalence of IBD (53.3%), followed by parents (26.7%), while offspring had the lowest prevalence (20%). Among the second-degree relatives, highest prevalence of IBD occurred in uncle-aunt (62.5%), followed by nephew-niece (25%) and grandparents (12.5%). The mean age of onset among family members was 29.2 years, the mean age at diagnosis was 30.5 years, and the duration of illness was 11.1 years. A relatively high proportion of affected family members (55%) had extensive colitis; 35% had extraintestinal manifestations and 16.6% had undergone surgery. Extraintestinal manifestations were present in 14 (48.27%) probands with UC and in 7 (35%) of the affected first-degree relatives (Table 3).
5. Concordance within Families
Concordance for extent of disease was found in half of UC families (50%). Similarly, concordance for extraintestinal manifestations was present in 9 of 18 UC families (50%). There was significant concordance for the mean duration of illness (63.8%, P=0.004); however, concordance was low for the mean age at onset (21.4%, P=0.3948) and the mean age at diagnosis (19.4%, P=0.400). Among the parent-offspring relations, the age at onset (43.3 years vs. 27.1 years) and age at diagnosis (44.6 years vs. 28.6 years) varied significantly, while there was little variation among siblings.
DISCUSSION
Familial aggregations of diseases provide unique insights into the pathogenesis. Both environmental and genetic factors underlie the familial occurrence of a disease. IBD shows familial aggregation, which is well reported in various studies. Familial occurrences in ethnically unique populations are different. Various Asian studies have reported that the familial aggregation of UC is far less than that in the West. A study from India reported a definite family history in 2.3% of patients with UC.17 Further studies in this regard are required from India and Asian countries. We undertook this study, therefore, to assess the prevalence of IBD among relatives of UC patients in India, and compared the baseline demographics as well as disease characteristics in familial and sporadic UC.
Of the 2,058 UC patients included in the study, a positive family history was found in 1.5%. This was much lower than the familial IBD prevalence of 5% to 18% reported from Western countries.1118192021 Among Asian populations, a study from Sri Lanka showed that a family history of IBD was present in 2.1% of UC patients,22 while a Japanese study reported 2.7%.15 In Korea, the prevalence of a positive family history of UC varied from 2.01% to 6.5%.142324 A Chinese study reported that 1.48% of UC patients had a family history, which is similar to the prevalence we saw in our study.25 This shows that the prevalence of familial UC is slightly lower in Asian countries as compared to the West. Familial aggregation includes genetic factors as well as environmental influences; as people from the same family may have similar lifestyles and share the same environment, they may also be affected by the same environmental exposure. Genetic mutations differ between different ethnic backgrounds. For example, the HLA-DRB1 alleles associated with UC differ between Asian and Western countries.2627282930313233 The NOD-2 mutation is not associated with CD in Japanese,34 Chinese,35 or Koreans,36 but an association has been identified in the Western populations.3738 Thus, this diversity helps to better elucidate the genetic component of the disease and to assess the role of heredity in the etiopathogenesis of IBD, which can help optimize genetic counseling in the future.
Our study showed a 100% concordance for the type of IBD among probands of UC and their family members, as compared with a previous study in which concordance was 70% for UC.39 However, in some other studies a high concordance for both types of the disease was found.124041 The disease susceptibility may therefore be specific, and patients with UC have a greater chance of a family member being affected by UC rather than CD.
In the present study, we investigated the differences in disease characteristics between patients with and without a family history. The proportion of male patients was significantly lower in familial cases (38.7%) as compared to sporadic cases (65.8%). However, the male to female ratio varied widely in different studies across populations.243942 The age at onset and diagnosis did not vary significantly between those with and without a family history in our study, unlike previous studies that showed a younger age at onset for familial UC cases.121524 Probands with a family history had a significantly lower proportion of extensive colitis (27.6% vs. 43.2%). Referral bias can explain the high proportion of extensive colitis and left-sided colitis in our study population. There were no significant differences in terms of outcomes such as surgery and use of medications, which is similar to the results of a study from South Korea.23
There are few data on similarities in UC families. A few studies report a high concordance for the extent of colonic involvement and presence of extraintestinal manifestations among family members.341 We arrived at similar conclusions in our study, with the concordance being 63.8% and 50% for extent of disease and presence of extraintestinal manifestations, respectively, in probands and their first-degree relatives. This further supports the view that UC arises in people with similar genetic or environmental predispositions.
In parent-offspring relationships, the ages at onset and diagnosis were found to be significantly lower in successive generations separated by more than 15 years in our study, but were almost the same among siblings. This could suggest a component of genetic anticipation in the development of UC. The concept of genetic anticipation implies an earlier onset and increased severity as the disease is passed through subsequent generations.43 However, no features of increased aggressiveness of disease were found in offspring compared with parents in our study.
We readily acknowledge a few limitations. This was a retrospective review of records of patients at a tertiary hospital. Therefore, the results may not be applicable to the general population. The clinical characteristics of first- and second-degree relatives were assessed mainly by telephonic interviews only. Having said this, the merits of our study are many. We included a large number of patients with UC from North India, and therefore enable a good estimate of the familial occurrence of IBD. Hence, there is direct clinical relevance, as the findings provide a risk estimate in our population, which will be invaluable in patient counseling.
In conclusion, a positive family history of IBD was confirmed in 31 (1.5%) of our patients with UC, which is lower than that reported from Western populations. All relatives of affected patients had UC and none had CD, showing a high concordance rate. The differences between various populations in familial aggregation may be due to either genetic or environmental factors. Studying these differences may help in better elucidating the etiopathogenic mechanisms of IBD.
 XML Download
XML Download