

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Crohn's disease (CD) is a chronic inflammatory digestive disease with a long-term course that is usually progressive, disabling, and relapsing, and most patients with CD undergo intestinal surgery during their lifetime.12 Effective therapy with immunomodulators and anti-tumor necrosis factor α antibody have the potential to change the natural course of CD. Actually, a large cohort study suggested that effective medical treatment has reduced the number of surgeries being performed for CD.3 On the other hand, intestinal strictures are still the main reason for surgeries such as intestinal resection and strictureplasty, which are performed to relieve stricture-related symptoms or ileus. Surgery is, however, not a basic treatment modality, and relapse at the anastomotic site is often a problem in CD.45 Surgery sometimes lead to stricture recurrence, with the need for repeat surgery, and frequent surgery can lead to short bowel syndrome.6 Endoscopic balloon dilation (EBD) is an alternative to surgery for strictures secondary to CD. This endoscopic treatment is mainly indicated for Crohn's strictures of the gastric outlet, duodenum, colon and, ileo-colonic anastomosis.789101112131415161718192021222324 Many reports concluded that EBD is effective and safe, and its use can avoid surgery. Moreover, balloon-assisted enteroscopy (BAE), including double-balloon enteroscopy and single-balloon enteroscopy have been widely used for diagnosis and endoscopic treatment of small bowel diseases.2526 Since BAE enables us to perform EBD for small bowel strictures in patients with CD, the indications for EBD in CD have increased.2728293031323334 Hence, it is important for gastroenterologists to know the current status and future direction of EBD for Crohn's strictures. This article reviews the literature on EBD performed using the traditional approach to strictures of the colon and ileo-colonic anastomosis, in addition to that on recent approaches to small bowel strictures using BAE.
EBD FOR COLORECTAL AND ILEO-COLONIC ANASTOMOTIC STRICTURES
1. Dilation Technique
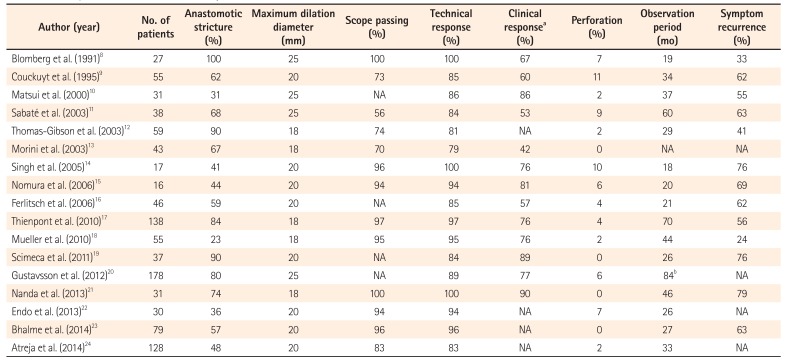
Two different EBD dilation catheters are used for gastrointestinal strictures: an over-the-wire balloon catheter and a through-the-scope balloon catheter. Through-the-scope balloon catheters tend to be selected for almost all EBD procedures because of their simplicity and safety. The length of the balloons for inflation is about 5 cm; therefore, stenoses 5 cm or longer are considered unsuitable for EBD. Moreover, intestinal strictures with deep ulcers and fistulous complications are contraindication for EBD. The dilation procedure is performed with monitoring of the pressure of the inflated balloon using a dilator under X-ray guidance. The maximum dilation diameter is selected at the discretion of the operating endoscopist. Table 1 shows a summary of published studies (only those that included 15 cases or more) on EBD using conventional colonoscopy in CD patients.89101112131415161718192021222324 In these 17 published studies, five used a maximum dilation diameter of 18 mm, eight used 20 mm, and four used 25 mm. Lower dilation pressure was thought to be a risk factor for earlier redilation in two studies.1116 On the other hand, Gustavsson et al.20 suggested that larger maximum dilation diameter (25 mm) in EBD was associated with complications such as perforation and hemorrhage. Therefore, when performing EBD, forcible dilation to achieve a larger dilation diameter or pressure is not recommended, as it could lead to intestinal perforation, and would require surgical intervention. Ideally, we should maximize the less invasive nature of EBD compared to surgery.
2. Short-Term Outcomes and Safety
A number of studies have evaluated the technical success and short-term clinical efficacy of EBD for Crohn's strictures. However, there are no standardized definitions of short-term success of EBD. Some authors simply defined successful dilation as technical response, while others defined successful dilation as disappearance of stenotic symptoms or ability to pass a scope as a technical response. The reported technical response rate ranged from 79% to 100%, whereas that using scope passage as the definition, which is the most obvious outcome, was 56% to 100%. Clinical efficacy was also determined based on the definition used in each study. Most investigators defined clinical efficacy as disappearance of stenotic symptoms, such as abdominal pain, nausea and abdominal boating. Recently, a visual analogue scale (VAS) has been used as a more strict evaluation method for confirmation of symptom relief.30 In published studies, clinical efficacy was achieved in 42% to 90% of patients.
The safety profile of EBD is important as a minimally invasive treatment. Perforation is one of the major concerns during this procedure, because it usually requires emergent surgery. No perforations were reported in four studies,13192123 although the remaining 13 studies reported perforations.891011121415161718202224 The rate of perforation was <10% in all but two studies,914 in which they were observed in 10% and 11% of subjects, respectively. EBD is thus recognized as a safe endoscopic treatment in patients with CD, since the short-term technical and clinical efficacy rates are relatively high and complication rates are low. Therefore, EBD for colorectal and ileo-colonic anastomotic Crohn's strictures may be as good a therapeutic option as surgical intervention, at least for the temporary relief of stenotic symptoms.
3. Long-Term Outcomes
Clinicians who treat CD patients with intestinal strictures should also be concerned about the long-term outcomes of EBD. Although this important outcome is generally assessed on the basis of symptom recurrence and surgery-free survival, in this review, only symptom recurrence was adopted as a criterion to evaluate long-term efficacy. The relapse rate of obstructive symptoms after EBD has been reported to be 24% to 79%. Approximately 60% of published studies reported that 50% or more of patients showed signs of relapse after initial EBD. In patients with recurrence of symptoms, redilation or surgical intervention should be performed. According to a meta-analysis that summarized 25 studies, including 1,089 patients and 2,664 dilations, the proportion of patients who required further dilation at 1, 2, and 5 years of follow-up was 31.6%, 25.9%, and 1.7%, respectively.35 Overall, the cumulative proportion of patients requiring further dilation over 5 years was 80.6%. Although EBD enables avoidance of surgery, the need for frequent redilation is a burden for both clinicians and patients. Hence, further information on patients who are likely to develop recurrence of symptoms is desirable. In fact, several studies have analyzed the predictors of redilation or surgery after EBD. Using stepwise logistic regression in a systematic review, Hassan et al.36 pointed out that stricture length of 4 cm or more was the only significant risk factor for recurrence (OR, 4.01; 95% CI, 1.16–13.8; P<0.028). On the other hand, other factors, such as the nature of strictures (naïve vs. postsurgical, active CD vs. inactive CD lesion), scope passage after EBD, and the method of graded dilation were not associated with treatment outcome.3536 Smoking is thought to be a risk factor for surgery after EBD.37 Thus, careful follow-up after EBD is needed for patients with risk factors.
4. Methods for More Effective and Safe EBD
Several reports described methods for more effective and safe EBD. Steroid injection into the stricture site after EBD was reported as a useful method for enhancing efficacy.3839 However, East et al.40 concluded that this method did not reduce the time to redilation after EBD of Crohn's ileo-colonic anastomotic strictures. Hence, further analysis including a large randomized controlled trial is essential to confirm the utility of steroid injection after EBD.
Carbon dioxide (CO2) insufflation is thought to be useful for the safe and smooth performance of EBD. CO2 insufflation is associated with rapid absorption resulting in less gas retention, which results in less pain during and after endoscopic treatment.414243 As EBD can be time-consuming, CO2 insufflation is more likely to have good short-term outcomes than air insufflation.44
EBD USING BAE FOR SMALL BOWEL STRICTURES
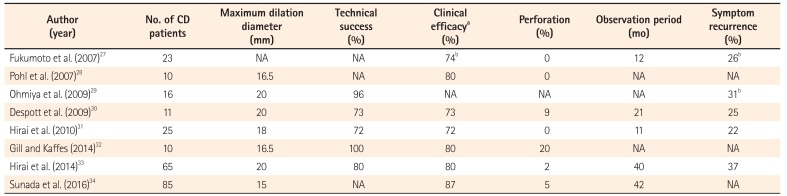
EBD using BAE for small bowel strictures is almost the same as EBD for colorectal and ileo-colonic strictures in terms of procedure and technique. However, special insertion techniques for deeper portions of the small intestine in BAE are necessary. Moreover, the proper insertion route should be determined according to the results of small bowel imaging. In addition, there are some technical difficulties, compared to EBD performed with a conventional colonoscope. For instance, it is not easy to stabilize the tip of the scope and to maintain a good visual field because of the limited space available, severe angulation, and adhesion in the small intestine. Therefore, EBD for small bowel strictures in CD is still challenging, although reports regarding this endoscopic intervention have recently increased, mainly from Japan (Table 2).2728293031323334 According to published studies, maximum dilation diameter for strictures of the small intestine varied from 15 mm to 20 mm which is relatively small compared to EBD for colorectal and ileo-colonic strictures. It is speculated that the reasons for the small dilation diameter are more severe strictures and the operator's concerns regarding perforation.
There are also no standardized definitions of short-term success of EBD for small bowel strictures. Despite the cited difficulties, the reported technical success rate is 72% to 100%, which is similar to the results of EBD for colorectal and ileo-colonic strictures. While clinical efficacy was evaluated based on the patient's obstructive symptoms in almost all studies, Despott et al.30 adopted the VAS score for abdominal pain in their evaluation. The clinical success rate was >70% (72%–87%) overall, which is comparable to published data on EBD for colorectal strictures. Perforations occurred in 0% to 10% of subjects in most published studies, although one small cohort reported a perforation rate of 20% (2/10).32 Judging from these results, EBD using BAE for small bowel strictures is equal to EBD using a conventional colonoscope in terms of short-term efficacy and safety.
There is insufficient reliable data on the long-term outcomes of the procedure for small bowel strictures, because the observation periods were very short, as shown in Table 2. However, in two studies that investigated the long-term outcomes of EBD for small bowel strictures, the average observation period after initial EBD was more than 3 years.3334 Hirai et al.33 reported that the cumulative surgery-free rate in 65 subjects was 79% and 73% at 2 and 3 years, respectively. However, the cumulative redilation-free rate in their analysis was 64% and 47% at 2 and 3 years. This rate was similar to the results reported in previous studies evaluating EBD for colonic and ileo-colonic anastomosis. Therefore, the need for frequent redilation seems to be an issue with EBD regardless of the target stricture site. According to a recent study published by Sunada et al.,34 the cumulative surgery-free rate after initial EBD for small bowel strictures in CD was 87.3% at 1 year and 78.1% at 3 years. Even though the cumulative surgery-free rate was similar to that in the study by Hirai et al.,33 they included patients with fistulas as subjects, and the presence of a fistula was significantly associated with the need for surgical intervention (hazard ratio, 5.50; 95% CI, 2.16–14.0; P=0.01). Hence, for small bowel strictures with fistula, EBD should be considered only in patients who are likely to benefit (e.g., for completion of important life events) from postponement of surgery.
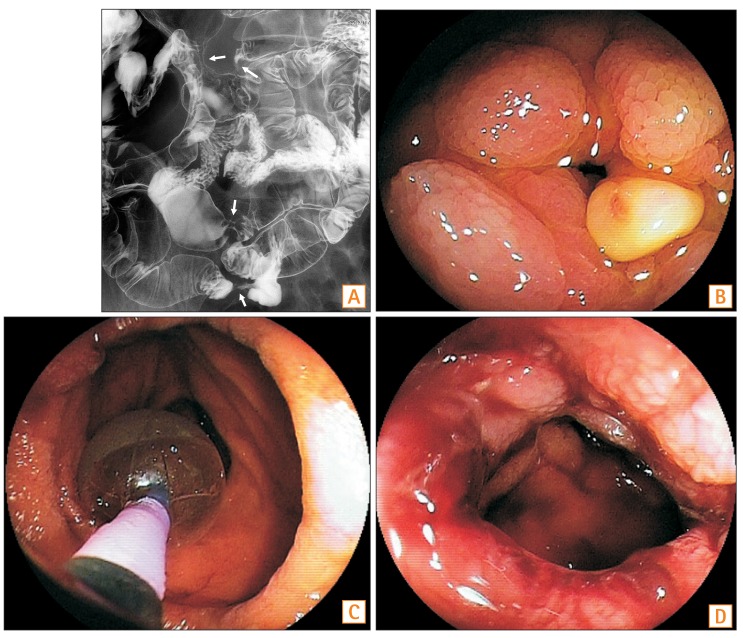
The tendency for CD patients to have multiple small bowel strictures is one of the limitations of EBD using BAE. In fact, the proportion of patients with multiple small bowel strictures was high in published studies. Although the therapeutic strategy for this situation is not established, in my opinion, in the absence of exclusion criteria such as fistulas, EBD can be attempted before performing surgery (Fig. 1). Further strict analysis will be needed for confirmation of efficacy of EBD for multiple small bowel strictures.
The disease behavior of CD has changed over time, with most patients having a stricturing type or a penetrating type.4546 In particular, since patients with ileal type CD tend to have small bowel strictures, performing EBD using BAE would be more meaningful to improve their quality of life. However, as described above, there is only limited evidence regarding the utility of this endoscopic intervention in patients with small bowel strictures. Further studies confirming the efficacy and safety of this procedure are desirable. In fact, a nationwide, multicenter, open-label, prospective cohort study is now ongoing in Japan. According to the results of interim analysis in this study, the short-term success rate using VAS score as an indicator was 69%, and no perforations were reported.47 The results also indicated equal efficacy and safety compared to published studies. The full data of this study will be published in the near future.
ISSUES AND FUTURE DIRECTIONS
Many issues should be addressed regarding EBD in CD. First, it is difficult to state whether EBD or surgery is best for release of intestinal strictures. Direct comparison between these two interventions is not easy, due to the differences in invasiveness and the goal of each treatment. Surgical interventions are superior to EBD in terms of certainty. According to a small retrospective cohort study, the proportion of patients who required any reintervention during follow-up was significantly lower in the surgical group than in the EBD group (OR, 5.62; 95% CI, 1.66–19.01; P=0.005).48 However, surgical interventions are inferior to EBD in terms of both the invasiveness and relapse at the anastomotic site. Strictureplasty has been performed for intestinal strictures in CD as a small bowel-saving strategy.49505152 Although the postoperative recurrence rate after strictureplasty is comparable to that of surgical resection, clinicians should also pay attention to the risk of malignancy in the preserved bowel. Since the performance of a randomized controlled study to compare EBD and surgical intervention is extremely difficult, gastroenterologists need to select an intervention method for intestinal strictures in CD by considering various factors (e.g., patients background, status of stricture, disease activity, length of small intestine, and so on) on a case by case basis.
The basic treatments for CD are not endoscopic or surgical interventions but medical therapies to control disease activity and improve quality of life. There are many effective medical treatments for CD, such as anti-tumor necrosis factor α antibody and immunomodulators. Additional candidates for treatments of CD will emerge in the future. Ideally, a combination of EBD and these effective medical treatments should be used for CD patients with intestinal strictures.
New endoscopic treatment modalities for Crohn's strictures such as the use of self-expanding metallic stents5354 and needle-knife treatment55 have been reported. Implantation of metallic stents has mainly been used for patients with malignant gastrointestinal strictures because these enable improved food intake without surgery. As EBD has the limitation of loss of long-term efficacy, stents have been used for Crohn's strictures in several institutions. However, there are some disadvantages, such as inflammatory reactions to a foreign body, recurrent stricture due to mucosal growth into the stent, and perforation or hemorrhage with self-expansion. Therefore, further large-scale studies to confirm the efficacy and safety of stenting are needed. Needle-knife treatment is a limited option for Crohn's stricture. With only a few case reports,5556 its efficacy is still uncertain and safety is questionable. Further experience is necessary in order to apply this intervention in CD patients with intestinal strictures.
 XML Download
XML Download