

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Dentigerous cysts are a common type of odontogenic cyst in the jaw that arise from degenerative changes in the enamel epithelium and are accompanied by an accumulation of fluid between the crown of the tooth and the lining epithelium1. They present as a single lesion, but bilateral or multiple lesions are usually found in patients with a developmental syndrome or systemic disease, such as Gorlin-Goltz syndrome (basal cell nevus syndrome), cleidocranial dysplasia, Maroteaux-Lamy syndrome, or mucopolysaccharidosis234. However, non-syndromic bilateral dentigerous cysts are very rare and we report a case of a 15-year-old male with bilateral dentigerous cysts that involved all four quadrants that had a symmetric appearance.
II. Case Report
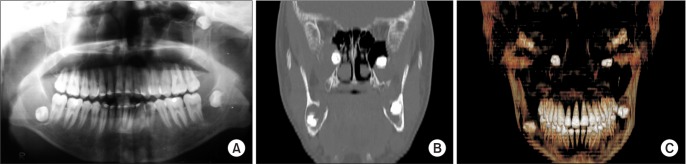
This case report was approved by the Institutional Review Board (HYI-15-102-1) of the Hanyang Univsersity Seoul Hospital and the patient provided informed consent. In January 2005, a 15-year-old male was referred to our clinic for asymptomatic multiple cystic lesions in both jaws, which were found by routine dental radiographs. The panoramic view revealed bilateral radiolucent cystic lesions around the unerupted mandibular third molars. In addition, well-defined radiolucent lesions were found in the superior-lateral aspects of both maxillary sinuses, which also contained the crowns of unerupted third molars.(Fig. 1. A) A computed tomography (CT) scan showed soft tissue masses obliterating both maxillary sinuses and displacing the maxillary third molars to the infraorbital area.(Fig. 1. B, 1. C) Both the patient and his parents were healthy without systemic disease or any signs of other syndromes. There were no abnormal findings in laboratory blood tests prior to the operation. Additionally, the chest radiograph was read as normal and did not show any in the clavicle and thorax areas.
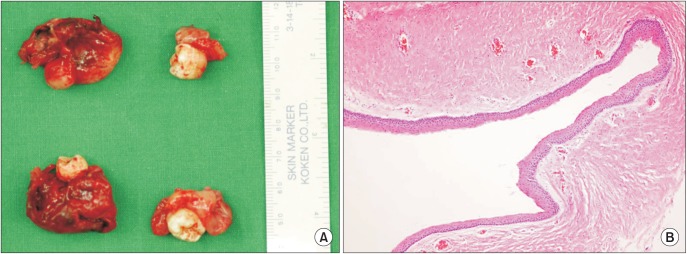
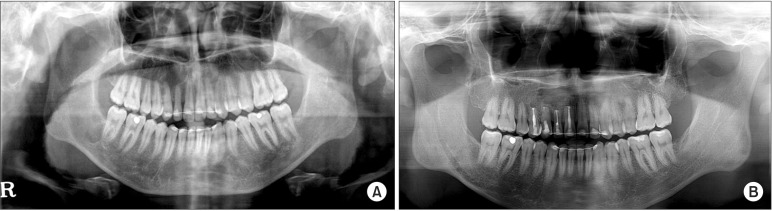
The bilateral cystic lesions in the maxilla were enucleated by the Caldwell-Luc approach; then, the mandibular third molars were removed by the gingival approach under general anesthesia in February 2005. All surgical specimens were unilocular cystic structures that contained a gray-yellowish material.(Fig. 2. A) Histopathologic analysis showed a typical dentigerous cyst lined by non-keratinized squamous epithelium with mild inflammatory cellular infiltration in the connective tissue.(Fig. 2. B) No dysplastic changes were observed. The patient was followed periodically for 10 years after surgery and no specific signs or symptoms related to the lesions in the operative sites were identified.(Fig. 3. A, 3. B)
III. Discussion
Dentigerous cysts are the most common type of developmental odontogenic cysts in the jaw and develop due to accumulation of fluid between the reduced enamel epithelium and the tooth crown, which leads to separation of the follicle from the crown of an unerupted tooth. They commonly arise from the mandibular third molars, maxillary canines, maxillary third molars, and mandibular second premolars1. A search of PubMed from 1943 to 2014 revealed that only 30 cases of bilateral dentigerous cysts in non-syndromic patients were reported; 24 cases occurred in the mandible, 3 in the maxilla, and 3 in both the mandible and maxilla56. Henefer7 reported a case of bilateral dentigerous cysts that simultaneously involved all four dental quadrants around the unerupted premolar and cuspids. However, in our case, the four dentigerous cysts involved un-erupted third molars and had a symmetric appearance in a non-syndromic patient.
The most common sites of dentigerous cysts are around the mandibular and maxillary third molars. The sites with high incidences of bilateral dentigerous cysts in nonsyndromic patients were similar to sites of general dentigerous cysts. The most common site was the mandibular third molar (11 cases), followed by the mandibular first molar (10 cases), maxillary third molar (2 cases), the maxillary cuspid (2 cases), mandibular first premolar (2 cases), mandibular second premolar (1 case), mandibular central incisor (1 case), and maxillary central incisor (1 case)56.
Early detection of dentigerous cysts can be challenging because it develops as an asymptomatic lesion before the increased size causes cosmetic or dental/sinus problems. In this case, the patient also presented with asymptomatic lesions, but routine dental examinations showed extensive maxillary cysts that extended to both orbital floors. Therefore, we suggest that when clinicians encounter similar cases of unerupted third molars, routine radiographic examination may help detect early dentigerous cyst lesions and an accurate diagnosis may prevent extensive surgery or complications.
Bilateral and multiple dentigerous cysts are usually found in association with a number of syndromes such as Gorlin-Goltz syndrome (basal cell nevus syndrome), cleidocranial dysplasia, and Maroteaux-Lamy syndrome234. Gorlin-Goltz syndrome is a rare autosomal dominant disorder characterized by variable manifestations, including multiple basal cell carcinomas, odontogenic keratocysts of the jaw, skeletal anomalies that include scoliosis and bifid ribs, palmar and plantar pits, calcification of the falx cerebri, and biparietal frontal bossing4. Cleidocranial dysplasia is a congenital disorder that causes skeletal abnormalities, i.e., delayed closures of cranial sutures and fontanelles, associated with the presence of wormian bone and clavicle aplasia. Oral manifestations include retention of deciduous teeth, multiple supernumerary teeth, delayed eruption or impaction of permanent teeth and formation of cysts around non-erupted teeth2. Maroteaux-Lamy syndrome results from a defect in specific lysosomal enzymes that are required for the degradation of specific mucopolysaccharides. Oral complications include unerupted dentition, detigerous cystic-like follicles, malocclusion and gingival hyperplasia3. Interestingly, there was one case of bilateral dentigerous cysts that was associated with a polymorphism in chromosome 1qh+8, and one case associated with long-term treatment with cyclosporine9.
In conclusion, it is important to identify patients with multiple or serial dentigerous cysts, and to investigate possible associated syndromes to prevent unnecessary complications. However, as we report in this case study, clinicians should confirm the extent of the cystic lesions using panoramic view and CT, even in a non-syndromic patient, and should keep the possibility of bilateral dentigerous cysts in mind in order to deliver accurate, early diagnoses.
 XML Download
XML Download