

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Acute loss of sensory function of the infraorbital nerve following orbitozygomatic complex fractures is often seen because of their close proximity as the nerve passes through the infraorbital sulcus in the floor of the orbit to exit through the infraorbital foramen1. Traumatic injury to the infraorbital nerve may be due to compression, edema, ischemia, or laceration2.
Persistent hypoesthesia following correction of mid-face and zygomatic complex fractures indicates injury to the infraorbital nerve. Although hyperesthesia along the distribution of the infraorbital nerve has been documented, it is comparatively rare in occurrence3,4. The incidence of long-term neurosensory deficits in different studies varies from 10% to 50%1,5.
The incidence of mid-face and zygomatic complex fractures presenting with fracture lines running through the inferior orbital foramen resulting in post-traumatic sensory disturbance has been well studied and documented through the years1,6,7,8,9. The most commonly documented cause for such sensory disturbance is nerve impingement by fractured segments which have been reduced or fixed inadequately2. This inaccessibility is compounded by the impeding course of the infraorbital nerve. The other cause is formation of fibrous or calcified tissue around the infraorbital nerve postoperatively, leading to nerve compression.
A review of literature provides strong evidence and varied methods for nerve decompression10,11. However the documented successful outcomes are not reported with individual techniques, which could result in temporary or permanent sensory loss.
To overcome this, we describe a new technique of repositioning the infraorbital nerve into the orbital floor before reduction and stabilization of the fractured zygomatic complex.
II. Materials and Methods
Two male and one female patients with history of road traffic accidents reported to the hospital emergency room. Clinical and radiological examination (Fig. 1) revealed a displaced zygomaticomaxillary complex fracture on the left side for one of the patients and on the right for another.(Fig. 2, 3) The third patient had a LeFort III fracture on the left and LeFort II
Surgical procedure
An intraoral approach was used to expose the zygomatic complex. Two percent lignocaine hydrochloride with adrenaline (1 : 80,000) was infiltrated at the site of incision. The incision was made in the buccal vestibule in the high mucobuccal fold area extending from canine to second molar region.
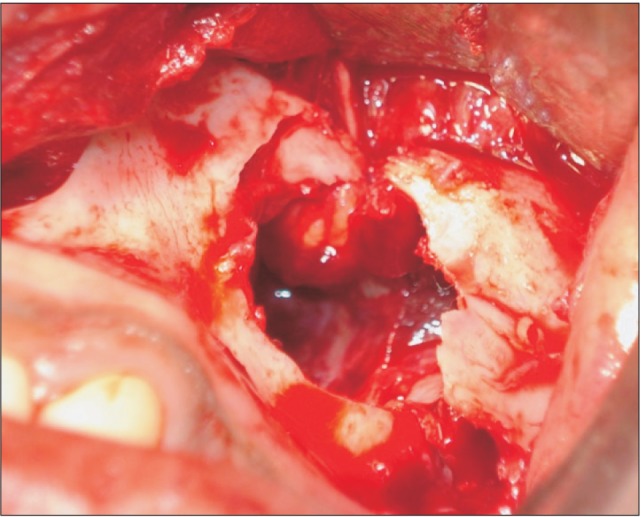
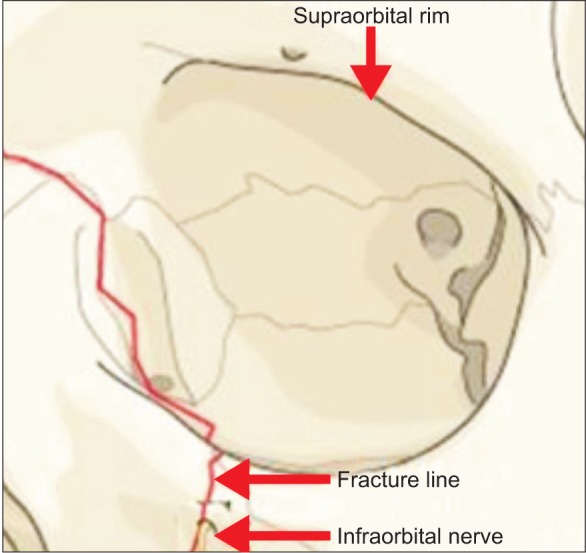
Sharp dissection was carried out subperiosteally to expose fractured segments in the infraorbital and zygomatic buttress region. The fracture line was seen running through the infraorbital foramen, and the neurovascular bundle was found entrapped between the fracture lines in the described cases.(Fig. 2, 3, 4)
With great care taken to minimize direct trauma to the infraorbital nerve, it was freed from the remnants of fractured foramen.(Fig. 5) Sharp bony spicules of the fractured segment impinging on the nerve were removed, and the nerve was dissected off the surrounding soft tissue along its long axis with the help of a nerve hook.(Fig. 6)
Then the nerve was mobilized sufficiently to check for any adhesions and was transpositioned to a higher level in the orbit at the floor level. This was done to gain access to the fracture lines for the placement of a fixation device near the infraorbital margin.
Rigid fixation of the zygomatic complex was achieved with titanium plates and screws.(Fig. 7) The surgical site was closed with continuous suturing using 3-0 vicryl suture material (Johnson & Johnson, Aurangabad, India), and patients were reversed and extubated uneventfully. Postoperatively, patients' eyes were examined using an orbital chart for signs of visual and sensory impairment.
The patients recovered uneventfully and had no evidence of sensory disturbance during their three-month follow-up.
Two-point discrimination testing was performed in the extraoral area of the infraorbital nerve distribution both preoperatively and postoperatively, and on both the affected and contralateral sides as a control.
The test was done separately on the lip and paranasal area using a caliper.
III. Results
There was no evidence of sensory disturbance during their three month follow-up in any of the patient.
IV. Discussion
Chronic sensory disturbance in the form of hypo- or hyperesthesia is a common postoperative symptom in patients with surgically repaired mid-face fractures1,4. In isolated posterior fractures, the infraorbital nerve may block the surgical field, preventing visualization of the fracture site. Rough dissection of this area may cause unexpected bleeding due to rupture of the orbital branch of the infraorbital artery12. These complications may cause surgeons to avoid manipulation around the nerve, which can lead to incomplete reduction of orbital floor fractures11. This, in turn, leads to restriction of ocular movement due to remnant entrapped periorbital tissue, and also postoperative enophthalmos due to undercorrection of the intraorbital volume11.
Although various operative alternatives have been tested to avoid these residual symptoms, satisfactory or definitive results have not been achieved8. Some studies advocate a secondary corrective surgery in such patients4.
We report three cases of mid-face trauma in which reduction of the fracture segment was performed after nerve transposition. This approach defers the need for a second surgery to correct post-traumatic sensory loss. Avoiding re-entry not only saves the patient's time and money, but also limits the edema and inflammatory response that may worsen nerve compression after a second surgery.
This approach also helps avoid additional transconjuctival incisions for approaching orbital fractures.
Moreover the placement and fixation of a miniplate after transposition is easy.
There was no difficulty in reducing the fracture after transposition of the nerve.
Hence, we recommend intraoperative transpositioning of the infraorbital nerve to the orbital floor in every mid-face fracture with fracture line running through the facial course of the nerve.





 XML Download
XML Download