

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
About 1,000 patients undergo aortic surgery annually in Korea. Unlike Western countries, emergency surgery for dissection or ruptured aneurysm is more frequent than elective cases. Because timely diagnosis and intervention are essential for improving the treatment outcome, medical professionals should be provided with accurate knowledge about the nature of the diseases and currently available treatment modalities along with their results. Aortic dissection is the most frequent among the acute aortic diseases. Although there is a wide variation in surgical results between hospitals, experienced centers are reporting early survival rates higher than 90% after a surgery for acute type A dissection. The majority of the patients with acute type B dissection can be treated medically. For those who have serious complications such as rupture or malperfusion, catheter-based intervention became a promising alternative to surgery. Aortic intramural hematoma and penetrating atherosclerotic ulcer are known to have better prognosis than dissection. However, treatment plans should be decided individually, because many of such lesions can progress into dissection or rupture. Because the result of surgery for ruptured degenerative aneurysm is poor, surveillance and timely intervention is of utmost importance. The mortality rate after elective aortic surgery has come into a satisfactory range; <10% for the thoracic and <5% for the abdominal aorta. Endovascular repair has been established as an effective treatment for the abdominal aortic aneurysm. However, its effectiveness and proper indications for thoracic aortic diseases are not fully determined. Refinement of device and combination with surgical repair (hybrid technique) will widen the indication of stent-grafting.
Figures and Tables
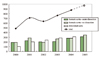

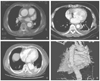
Figure 3
Computed tomographic scan images of various malperfusion syndrome caused by aortic dissection.
(A) True lumen compression in right common carotid artery causing stroke.
(B) Obstruction of arch branches by mobile intimal flap causing cerebral ischemia and arm ischemia.
(C), (D) Malperfusion of left main coronary artery causing acute myocardial infarction.
(E), (F) Occlusion of superior mesenteric artery causing bowel infarction.





References
1. Kim YW. Report of nation-wide questionnaire survey for abdominal aortic aneurysm treatment in Korea. Korean J Vasc Surg. 2005. 21:10–15.
2. Beaver TM, Herrbold FN, Hess PJ, Klodell CT, Martin TD. Transferring diagnosis versus actual diagnosis at a center for thoracic aortic disease. Ann Thorac Surg. 2005. 79:1957–1960.

3. Svensson LG, Kouchoukos NT, Miller DC. Expert consensus document on the treatment of descending thoracic aortic disease using endovascular stent-grafts. Ann Thorac Surg. 2008. 85:S1–S41.
4. Suzuki T, Mehta RH, Ince H, Nagai R, Sakomura Y, Weber F, Sumiyoshi T, Bossone E, Trimarchi S, Cooper JV, Smith DE, Isselbacher EM, Eagle KA, Nienaber CA. International Registry of Aortic Dissection. Clinical profiles and outcomes of acute type B aortic dissection in the current era: lessons from the international registry of aortic dissection (IRAD). Circulation. 2003. 108:S1. II312–II317.
5. Hata M, Shiono M, Inoue T, Sezai A, Niino T, Negishi N, Sezai Y. Optimal treatment of type B acute aortic dissection: long-term medical follow-up results. Ann Thorac Surg. 2003. 75:1781–1784.
6. Yu HY, Chen YS, Huang SC, Wang SS, Lin FY. Late outcome of patients with aortic dissection: study of a national database. Eur J Cardio-thorac Surg. 2004. 25:683–690.
7. Olsson C, Eriksson N, Stahle E, Thelin S. Surgical and long-term mortality in 2634 consecutive patients operated on the proximal thoracic aorta. Eur J Cardio-thorac Surg. 2007. 31:963–969.
8. Westaby S, Bertoni GB. Fifty years of thoracic aortic surgery: lessons learned and future directions. Ann Thorac Surg. 2007. 83:S832–S834.
9. Westaby S, Saito S, Katsumata T. Acute type A dissection: conservative methods provide consistently low mortality. Ann Thorac Surg. 2002. 73:707–713.
10. Bavaria JE, Brinster DR, Gorman RC, Woo YJ, Gleason T, Pochettino A. Advances in the treatment of acute type A aortic dissection: an integrated approach. Ann Thorac Surg. 2002. 74:S1848–S1852.
11. Geirsson A, Szeto WY, Pochettino A, McGarvey ML, Keane MG, Woo YJ, Augoustides JG, Bavaria JE. Significance of malperfusion syndrome prior to contemporary surgical repair for acute type A dissection: outcomes and need for additional revascularizations. Eur J Cardio-thorac Surg. 2007. 32:255–262.
12. Watanuki H, Ogino H, Minatoya K, Matsuda H, Sasaki H, Ando M, Kitamura S. Is emergency total arch replacement with a modified elephant trunk technique justified for acute type A aortic dissection? Ann Thorac Surg. 2007. 84:1585–1591.
13. Halstead JC, Spielvogel D, Meier DM, Rinke S, Bodian C, Malekan R, Ergin MA, Griepp RB. Composite aortic root replacement in acute type A dissection: time to rethink the indications? Eur J Cardio-thorac Surg. 2005. 27:626–633.
14. Geirsson A, Bavaria JE, Swarr D, Keane MG, Woo YJ, Szeto WY, Pochettino A. Fate of the residual distal and proximal aorta after acute type A dissection repair using a contemporary surgical reconstruction algorithm. Ann Thorac Surg. 2007. 84:1955–1964.
15. Kato M, Kuratani T, Kaneko M, Kyo S, Ohnishi K. The results of total arch graft implantation with open stent-graft replacement for type A aortic dissection. J Thorac Cardiovasc Surg. 2002. 124:531–540.
16. Sakaguchi G, Komiya T, Tamura N, Kimura C, Kobayashi T, Nakamura H, Furukawa T, Matsushita A. Patency of distal false lumen in acute dissection: extent of resection and prognosis. Interactive Cardiovasc Thorac Surg. 2007. 6:204–208.
17. Kusagawa H, Shimono T, Ishida M, Suzuki T, Yasuda F, Yuasa U, Onoda K, Yada I, Hirano T, Takeda K, Kato N. Changes in false lumen after transluminal stent-graft placement in aortic dissections. Six years' experience. Circulation. 2005. 111:2951–2957.
18. Czerny M, Zimpfer D, Rodler S, Funovics M, Dorfmeister M, Schoder M, Marta G, Weigang E, Gottardi R, Lammer J, Wolner E, Grimm M. Endovascular stent-graft placement of aneurysms involving the descending aorta originating from chronic type B dissections. Ann Thorac Surg. 2007. 83:1635–1640.
19. Vilacosta I, San Roman JA. Acute aortic syndrome. Heart. 2001. 85:365–368.
20. Neri E, Capannini G, Carone E, Diciolla F, Sassi C. Evolution toward dissection of an intramural hematoma of the ascending aorta. Ann Thorac Surg. 1999. 68:1855–1856.
21. Von Kodolitsch Y, Csösz SK, Koschyk DH, Schalwat I, Loose R, Karck M, Dieckmann C, Fattori R, Haverich A, Berger J, Meinertz T, Nienaber CA. Intramural hematoma of the aorta. Predictors of progression to dissection and rupture. Circulation. 2003. 107:1158–1163.
22. Song JK, Kim HS, Kang DH, Lim TH, Song MG, Park SW, Park SJ. Different clinical features of aortic intramural hematoma versus dissection involving the ascending aorta. J Am Coll Cardiol. 2001. 37:1604–1610.
23. Park KH. Prevalence of intimal defect in the patients with surgically treated acute type A intramural hematoma of the aorta. Korean J Thorac Cardiovasc Surg. 2007. 40:733–744.
24. Cho KR, Stanson AW, Potter DD, Cherry KJ, Schaff HV, Sundt TM 3rd. Penetrating atherosclerotic ulcer of the descending thoracic aorta and arch. J Thorac Cardiovasc Surg. 2004. 127:1393–1399.
25. Grabenwoger M, Fleck T, Czerny M, Hutschala D, Ehrlich M, Schoder M, Lammer J, Wolner E. Endovascular stent graft placement in patients with acute thoracic aortic syndromes. Eur J Cardiothorac Surg. 2003. 23:788–793.
26. Elefteriades JA. Natural history of thoracic aortic an: indications for surgery, and surgical versus nonsurgical risks. Ann Thorac Surg. 2002. 74:S1877–S1880.
 XML Download
XML Download