

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a systemic non-inflammatory, musculoskeletal disorder characterized by calcification of various entheseal sites of the body [1]. The reported prevalence of DISH is higher among elderly and predominantly seen in males [23]. In comparison to ankylosing spondylitis and other ankylosing disorders, there is limited data available on DISH. It usually manifests as an asymptomatic condition with mild symptoms [4]. It is well known to be associated with serious clinical manifestations viz. myelopathy, radiculopathy, vertebral canal stenosis, spinal cord injury subsequent to spinal fracture, complete spinal ankyloses, cervical airway obstruction, entrapment of peripheral nerves and dysphagia [5678].
Recently DISH has drawn increasing attention among researchers and clinicians. Although DISH is considered as an asymptomatic condition, increasing evidence suggests that it is an important indicator of underlying pathological osseous changes. DISH progression may alter the biomechanics of the spine, which subsequently results in several serious complications [5678]. In spite of its increasing clinical significance, the prevalence of DISH is largely unknown in most of the Asian countries.
The etiology of the disease lacks clarity. Various factors have been hypothesized to be involved in the pathogenesis of DISH such as exposure to environmental factors (retinol and fluoride), mechanical factors, genetic factors (human leukocyte antigen genes), excess growth factors (insulin-like growth factor), obesity and type 2 diabetes, mellitus and drugs (vitamin A derivatives, acitretin, isotretinoin, and etretinate) [91011121314]. Current theories suggest that calcification of anterior longitudinal ligament is due to the altered function and growth of the osteoblasts [15].
Clinically the diagnosis of DISH is made using radiological investigations and based on following criteria; presence of ossified or calcified ligament over at least four contiguous vertebrae, no significant degenerative changes in the intervertebral disc with preservation of its relative height in the affected areas, complete absence of sacroiliac or apophyseal joint ankyloses and non-fusion of intraarticular areas [2]. DISH is often seen in the thoracic region, followed by cervical and lumbar regions [16].
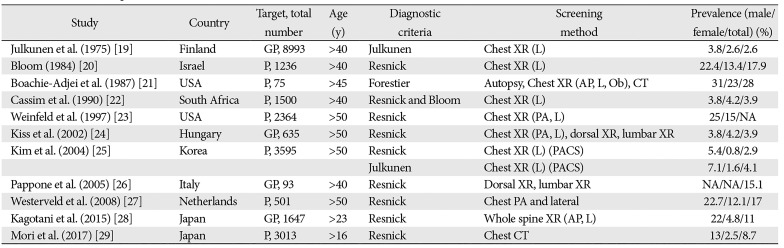
There is no established successful treatment available for the disease. Physical therapy, anti-inflammatory medication, analgesics, and sedation are reported to be effective in the management of the disease [1718]. The prevalence of DISH has been explored in different populations all over the world, including in Asian population (Table 1) [1920212223242526272829]. DISH studies in literature have studied samples from above 40 to 50 years of age (Table 1). To the best of our knowledge, only one study has been conducted in Middle East region more than three decades ago [20]. The total number of general X-ray (plain Xray and intravenous urogram) at Department of Radiology, Sultan Qaboos University Hospital (SQUH) as per last report available is 47,021 [30]. Of these only plain chest X-rays of those over 50 years in the year of study was 6,500. The database was readily available to conduct this first study in Oman to determine the prevalence of DISH and its associated factors in Omani elderly population.
Materials and Methods
This retrospective study is based on the compilation of relevant information from the Track Care database of SQUH related to all indoor and outpatients aged more than 50 years referred for chest X-ray to Department of Radiology, SQUH, from January 2016 to December 2016. These patients were included in the study. The age and sex of the patients were documented. Patients with inconclusive chest X-rays, history of spinal fractures were excluded from the study. The posteroanterior and lateral chest radiograms of these patients were reviewed by the same radiologist using Picture Archiving and Communication System (PACS, ver. 4.4.516.21), manufactured by Philips Company (Foster City, CA, USA). The diagnosis of DISH was based on Resnick's definition [2]. The positive cases of DISH were established when there was a contiguous ossified ligament over at least four consecutive vertebrae. Presence of three level involvement of ossification was considered as pre-stage DISH [27]. Assuming a DISH prevalence of 20% in our population, the sample size calculated for a single proportion for a finite population, considering relative precision of 10% was 1,223. Institutional Ethical Committee (SQU-EC/093/17) has approved the study.
Statistical analysis
The data was analyzed using SPSS Statistics software ver. 23 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to describe the distribution pattern of DISH among different age groups and sex. The association between DISH with age and gender was determined using Chi square analysis. Logistic regression was performed to determine the odds of age and sex with DISH.
Results
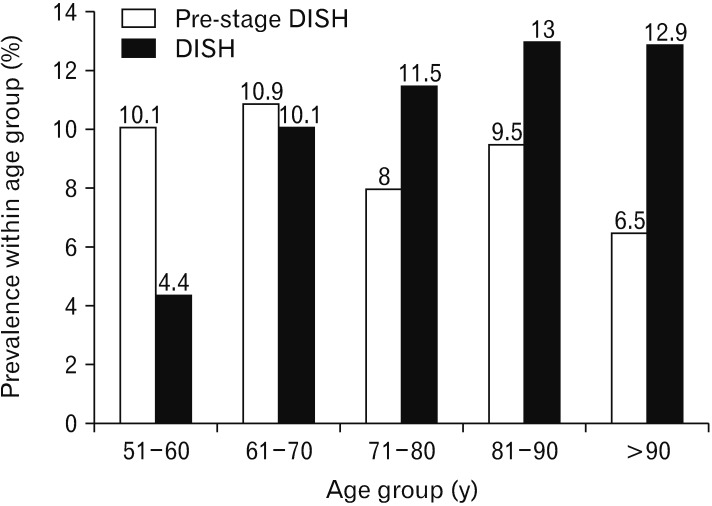
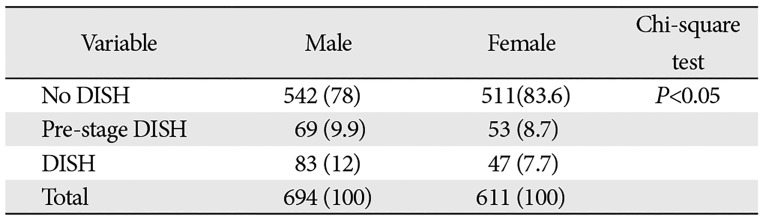
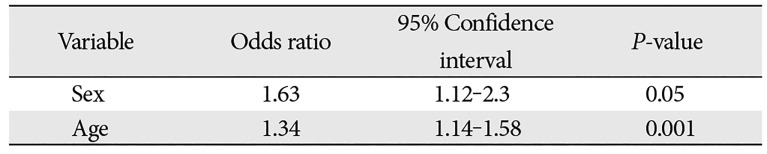
A total of 1,305 patients referred for chest X-ray to SQUH in Oman were included in the study. Among the study subjects, 694 (53.2%) were men. The overall prevalence of DISH in the cohort was 10% (n=130). The DISH prevalence was more frequent in men (n=83, 12%) than in women (n=47, 7.7%) and male to female ratio was 1.56:1. The overall prestage DISH prevalence was 9.3% (n=122) and male to female ratio was 1.14:1. Age (chi-square=14.6, df=4, P<0.05) and sex (chi-square=6.5, df=1, P<0.05) were found to be significantly associated with DISH. The DISH prevalence significantly increased with increasing age from 4% to 13%, except for >90s age group where it remained constant (12.9%). The odds ratio for gender and increasing age was 1.63 (95% confidence interval [CI], 1.12–2.3; P<0.05) and 1.34 (95% CI, 1.14–1.58; P<0.001), respectively. These results indicate that elderly men are more prone to develop DISH (Tables 2, 3, Figs. 1, 2).
Discussion
DISH was recognized few decades ago and was described with various synonyms. Initially, in 1938 Meyer and Forester [31] introduced the term moniliform hyperostosis to describe the thoracic spine hyperostosis and calcification. In 1950, Forestier and Rotes-Querol [1] used another term senile ankylosing vertebral hyperostosis or ‘Forestier's disease’ to differentiate it from other spinal diseases. Later in 1975, Resnick et al. [2] introduced the term DISH to describe the disease more appropriately. They have proposed a diagnostic criterion for DISH after their study on spines of 215 cadavers and 100 patients. Most of the clinicians and researchers have used Resnicks's criteria to diagnose DISH (Table 1), but few authors have also used Julkunen's and Utsinger criteria [1932].
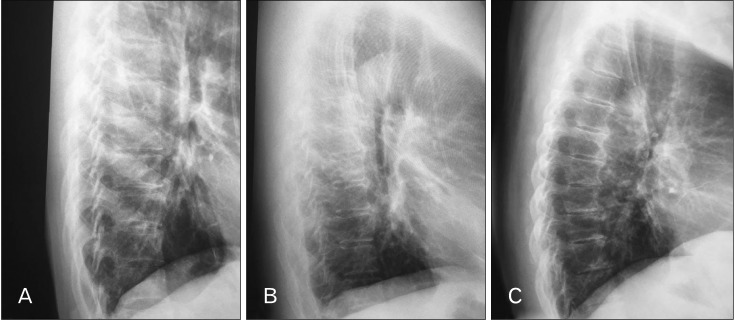
Most of the studies have used plain chest X-rays (posteroanterior and lateral chest X-rays) as screening method (Table 1). Few authors have preferred cadaveric autopsy [21], computed tomographic scan [29] and magnetic resonance imaging [33]. In our study, lateral chest X-rays were reviewed. In our study lateral chest X-rays were reviewed mainly because DISH was found to be more prevalent in thoracic spine. Also chest X-ray investigations have better patient acceptability, are convenient and readily available, have low amount of radiation, are safe and the findings are relatively consistent. Furthermore, it has been demonstrated that the lateral chest X-rays have relatively high specificity and sensitivity [31]. In our study, screening of chest X-rays was carried out on PACS system. PACS presents the complex data in simplified manner and images can be stored indefinitely and retrieved on request [34].
The prevalence of the DISH has been reported in various selected populations all over the world (Table 1). Weinfeld et al. [23], have studied the prevalence among different ethnic groups including white, Asian, black, native-American, and Hispanic population and have noted a low prevalence in Asians. Further, they concluded that genetic and/or hereditary difference could influence the prevalence of the DISH. Utsinger also described such influence based on the findings on Prima Indians from Arizona [32].
The prevalence of DISH in Asian population is variable in comparison to other ethnic groups and/or Western population. Among Asians, in Koreans the reported prevalence is 2.9% to 4.1% according to different criteria used for diagnosis [25]. In Jewish population from the Middle East [20], a higher prevalence of 22.4% among men and 13.4% among women has been documented. Two studies in Japan noted prevalence estimates of DISH as 11% [28] and 8.7% [29]. The prevalence in the present study (11%) is lower than Jewish population and higher than Koreans, but nearly similar to Japanese. In European countries, the prevalence of DISH varied between 2.6 % and 17% [19242627]. Prevalence of DISH in Oman is lower than Italy [26] and Netherlands [27] but it is much higher than Finland [19] and Hungary [24].
Even though the pathogenic process of DISH begins at early part of life, the disease is observed most commonly in elderly people older than 40 years of age (Table 1). However, the evidence suggests that although calcification of enthuses beings between 20 to 40 years of age, the complete progression of disease to fulfil the diagnostic criteria requires several decades [3]. In a study by Mata et al. [35], the disease was reported in population older than 70 years of age. Holton et al. [36], have reported high prevalence in men aged older than 65 years. Cassim et al. [22] demonstrated that patients older than 70 years would have prevalence higher than 10%. In a study by Henrard and Bennett [37], prevalence increased to a maximum of 54 in men and 14% in women aged 65 years. Bloom [20] have noted an increased trend in prevalence with increasing age to a maximum of 46% in males and 30% in females aged 80 years. Weinfeld et al. [23] compared the prevalence at two different age groups (50 and 70) and found approximately 10% increase in prevalence with increasing age. From the above reports, it is clear that the prevalence and age are positively correlated. Similar to previous reports in the present study prevalence increased with increasing age. With regard to the available evidence, the well-known male dominance is also being seen in our study. However, it is lower than the expected male/female ratio of 2:1 [3].
In our study, we have recorded the pre-stage DISH to understand the progression and natural course of the disease. In Netherlands population, Westerveld et al. [27], have found that pre-stage DISH was more frequent in women and raised with increasing age. Their findings suggested that women most likely develop ligament ossification at a later life but does not progress into a complete DISH. Contrary to their findings, in our results pre-stage DISH was found to be more frequent in men and was not influenced by age. There is a need for more studies to draw inference for conclusive evidence regarding the same.
Our findings need to be interpreted with caution. Our study being single-centered, there is a possibility of underestimation of prevalence due to selection bias in our study, as we included only those subjects who underwent radiological investigation at this center, and this sample may not be representative of all the elderly subjects.
Prevalence of DISH in Oman is lower than in Jewish population, almost similar to Japanese but higher than in Koreans. It may perhaps support the hypothesis that ethnic factors influence the DISH prevalence. In addition, DISH prevalence is positively associated with age and gender in our study. We recommend that appropriate precautionary measures need to be taken to target the ageing population, with special emphasis on elderly men.
 XML Download
XML Download