

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Celiac trunk is the first ventral branch from the abdominal aorta immediately below the aortic orifice of the diaphragm. It passes almost horizontally and towards right just superior to the pancreas and splenic vein, dividing into classical three branches: left gastric, common hepatic and splenic arteries. Variations in the branching pattern of the celiac trunk have been reported by many authors [1]. However, the absence of the celiac trunk is a very rare arterial variation (0.38%) [2] that has not been reported in many of the classical studies [34]. Between the presence of a complete celiac trunk pattern (84%) and the absence of the celiac trunk (<1%) there is an incomplete celiac trunk group (9%) [1]. The incomplete celiac trunk group has been classified into different types: (1) hepatosplenic trunk (5%), (2) gastrosplenic trunk (3%), (3) gastrohepatic trunk (1%), and (4) no trunk formation (less than 1%) [1]. On the other hand, the presence of hepatomesenteric trunk has been reported varying from 0.5% to 3.5% [5]. But according to an Indian study by Binit Sureha et al. [6], the incidence of hepatomesenteric trunk was 1.0% (6 in 600 patients). The knowledge of such variations is important during surgery like liver transplantation, pancreaticoduodenectomy, as well as during hepatic artery infusion chemotherapy. Similarly, dorsal pancreatic artery arising from celiac trunk is a rare variation, seen only in 33% of cases. Middle colic artery arising from celiac trunk is also rare variation, seen only in 1.2%–4.8% of cases [7]. Because of anomalous origin of these arteries there will be variation in the arterial supply of the pancreas and the colon. Knowledge of anomalous origin of arteries is essential for successful pancreas transplant and in hemicolectomy surgeries.
Materials and Methods
This study was performed on 20 formalin fixed abdomen specimens in the Department of Anatomy, Jagadguru Sri Shivarathreeshwara Medical College, Mysuru, Karnataka. The study was conducted during routine dissection for I MBBS. The abdomen was opened and celiac trunk was dissected according to Cunningham's manual and variations in the celiac trunk were observed and photographed.
Results
During routine dissection of abdomen for undergraduates, we observed the following variations in the branching pattern of celiac trunk.
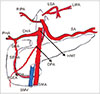
Total absence of celiac trunk associated with an hepatomesenteric trunk
Absence of celiac trunk is when all the three branches of celiac trunk arise independently from the abdominal aorta (Fig. 1). In the present case, the left gastric artery was arising as the first ventral branch directly from abdominal aorta. The splenic artery was arising as the second ventral branch directly from abdominal aorta 0.5 cm below the origin of left gastric artery. The dorsal pancreatic artery of the splenic artery passed dorsal to the pancreas and after crossing the superior mesenteric vessels anteriorly terminated by joining the junction of anastomoses between the ventral branches of superior and inferior pancreaticoduodenal arteries forming Kirk's arcade.
The hepatomesenteric trunk was arising as the third ventral branch from abdominal aorta 1 cm below the origin of splenic artery and gave rise to common hepatic and superior mesenteric arteries. Common hepatic artery was 5 cm long, passing anterior to portal vein above the first part of duodenum, divided into proper hepatic and gastroduodenal arteries. Proper hepatic artery immediately divided into right and left hepatic arteries.
The gastroduodenal artery after passing posterior to the first part of the duodenum continued as superior pancreaticoduodenal artery, which divided into ventral and dorsal branches anastomosing with the similar branches of inferior pancreaticoduodenal artery, branch of the superior mesenteric artery. The right gastroepiploic artery was arising from the junction of anastomoses between the ventral branches of superior and inferior pancreaticoduodenal arteries. The right inferior phrenic artery was arising from the splenic artery and the left one from the left gastric artery.
Quadrifurcation of celiac trunk with dorsal pancreatic artery arising from it
Dorsal pancreatic artery after taking origin from celiac trunk passed posterior to the body of pancreas and splenic vein and ended by supplying pancreas (Fig. 2).
Quadrifurcation of celiac trunk with middle colic artery arising from it
Middle colic artery arising from the celiac trunk passed posterior to the body of the pancreas and splenic vein and divided into three branches after it entered transverse mesocolon (Fig. 3).
Left inferior pheric artery arising from celiac trunk
Left inferior phrenic artery was arising as first direct branch from celiac trunk (Fig. 4). Left gastric artery as second branch and celiac trunk continued as hepatosplenic trunk dividing into common hepatic and splenic arteries.
Highly tortuous splenic artery giving an additional branch to transverse colon
The course of the splenic artery was highly tortuous and retropancreatic, gave an additional branch to distal 1/3rd of transverse colon before it entered the hilum of spleen (Fig. 5).
Discussion
Absence of celiac trunk is one of the rarest anomaly of the celiac trunk, has been reported by several authors [891011]. According to Matusz et al. [12], absence of celiac trunk was observed only in 0.19% of cases, incomplete celiac trunk was observed in 6.09% of cases and complete celiac trunk was present in 90.7% of cases.
The presence of hepatomesenteric trunk has been reported in 2.5% of cases [4], 3% of cases [1], 3.5% of cases [5]. But according to angiographic study report by Koplay and Kantarci [13], it is rare for a common hepatic artery to take origin from superior mesenteric artery with a 0.86% or from the aorta (0.43%) in angiograms of 701 patients. According to Ghosh [14], in a cadaveric study of 125 livers, reported classical trifurcation of the celiac trunk in 123 cases and hepatomesenteric trunk only in two cases along with bifurcation of the trunk as splenogastric trunk [14].
Nakamura et al. [15] also reported three cases of gastrosplenic with hepatomesenteric trunks.
In the present study, hepatomesenteric trunk was not associated with splenogastric trunk that is why it is very rare variation.
According to latest cadaveric study by Olewnik et al. [16], on 40 cadavers, six types of coeliac trunk branching patterns were reported. Accessory hepatic arteries in seven specimens (17.5%), normal trifurcation, accounting for 62.5% of cases, quadrifurcation with right accessory hepatic artery from celiac trunk, trifurcation with common hepatic artery, splenic artery, and right accessory hepatic artery. The rarest variation was absence of the coeliac trunk, with an incidence of 2.5%. In this variation, the left gastric artery, the common hepatic artery, and the splenic artery branched directly off the abdominal aorta [16].
The blood supply of liver as described in standard textbooks by proper hepatic artery was seen in 79.1% of cases. Aberrant right hepatic artery in 11.9%, aberrant left hepatic artery in 3.0%, hepatic arteries arising from aorta or double hepatic arteries from celiac trunk in 4.1% of cases in 604 patients who underwent angiographies of celiac and superior mesenteric arteries according to study conducted by Koops et al. [17]. According to Rammohan et al. [18], the commonest variations in the blood supply of liver are the replaced right hepatic artery (11%–21%), replaced left hepatic artery (3.8%–10%) and rarest is by hepatomesenteric trunk (<1%). When common hepatic artery originates from hepatomesenteric trunk, it can pass either above the pancreatic head (suprapancreatic), below the uncinate process of pancreas (infrapancreatic) or through the substance of pancreas (transpancreatic) [18]. In the present case, common hepatic artery was suprapancreatic and passing anterior to the portal vein [19]. Apart from the branches mentioned above which supply the liver, Ghosh [14] mentioned the importance of the middle hepatic artery in living donor liver transplantation in his study. He noticed in 19 (15.2%) livers that in the presence of an accessory left hepatic artery, the middle hepatic artery arose from the right hepatic artery. Presence of the above hepatic arterial pattern in the donor could possibly increase the risk of intraoperative injury to the middle hepatic artery during living donor liver transplantation. Injury to the hepatic arterial system could lead to severe complications like hepatic artery thrombosis, which may result in graft loss or reduction in the blood supply to the remaining liver in the donor or both [14]. The anatomical variations of the coeliac trunk are due to developmental changes in the ventral segmental arteries. Primitive segmental branches arise from the dorsal aorta and form the celiac trunk and the superior mesenteric artery. These branches are connected to the ventral longitudinal anastomotic channel. Retention or disappearance of parts of this primitive arterial plexus will give rise to variations of the celiac trunk and the superior mesenteric artery [172021].
Moreover, in the present case right and left inferior phrenic arteries were arising from the left gastric and splenic arteries respectively. Left gastric arising from abdominal aorta has been reported by Lipshutz [22] in 15% of cases. Left gastric giving left inferior phrenic artery was reported by Piao et al. [23], to be in 2.9% of cases.
But right inferior phrenic artery arising from splenic artery not mentioned in the literature This is the first time to report a case of absence of celiac trunk associated with an hepatomesentric trunk and independent origin of left gastric and splenic arteries from the abdominal aorta in South Indian area (Fig. 6).
The dorsal pancreatic artery was first described by Haller (1745) [7]. It is the main artery supplying blood to the tail of pancreas together with the splenic artery, so one of the most important artery highly selected for pancreatic angiography. It usually arises from splenic artery (37%), celiac trunk (33%) superior mesenteric artery (21%) and common hepatic artery (8%). It arises from the suprapancreatic segment of the splenic artery runs dorsal to neck of pancreas [5]. It runs downwards to the inferior border and divides into terminal branches. Right branches anastomose with the pancreatic arcades formed by the superior and inferior pancreaticoduodenal arteries, left branch also called transverse pancreatic artery runs along the inferior edge of the gland towards the tail of the pancreas.
Sometimes dorsal pancreatic artery forms the anterior and posterior pancreaticoduodenal arcades with superior pancreaticoduodenal arteries, when inferior pancreaticoduodenal artery is absent from superior mesenteric artery. In such case major portion of the pancreas is supplied by the dorsal pancreatic artery [24]. Damage to the dorsal pancreatic artery is more common when dorsal pancreatic artery arises from the common hepatic artery or celiac trunk, instead of the splenic artery, resulting in an unintentional damage to the pancreatic graft. Attempts should be made to revascularize the graft through the cut dorsal pancreatic artery [25].
Middle colic artery usually arises from the superior mesmesenteric artery, just below the uncinate process of the pancreas. It passes inferiorly and enters the root of the transverse mesocolon and divides into right and left branches anastomosing with the ascending branches of right colic and left colic arteries respectively forming a portion of marginal artery which supplies the colon. The transverse colon receives its blood supply from the superior and inferior mesenteric arteries. But in the present case the middle colic artery originating from the coeliac trunk supplied the transverse colon instead of the superior mesenteric artery. There was no middle colic artery coming from the superior mesenteric artery. It divided into three branches before supplying the transverse colon in the transverse mesocolon [26]. The right branch was anastomosing with the ascending branch of right colic artery supplying hepatic flexure, middle branch was anastomosing with right and left branches and supplying the transverse colon. Yíldírím et al. [27] reported a case of anomalous origin of middle colic artery from celiac trunk. According to Bergman's, middle colic artery can arise from coeliac trunk in 1.2%–4.8% of cases. According to Amonoo-Kuofi et al. [28], in case of anomalous origin of middle colic artery, the only contribution of the superior mesenteric artery to the marginal artery will be ileocolic and right colic arteries, making ascending colon and transverse colon susceptible for increased vascular damage. In case of accessory left colic arteries from the superior mesenteric artery, the major portion of the marginal artery is contributed by the superior mesenteric artery which supplies even the splenic flexure and proximal part of descending colon [28]. But in the present case there was no left colic branch from inferior mesenteric artery nor accessory left colic arteries from the superior mesenteric artery. The main left branch of middle colic after passing posterior to the transverse colon was anastomosing with the ascending branch of first sigmoidal artery. The primary arterial supply for the splenic flexure and distal third of the transverse colon is left colic artery. But the left branch of the middle colic can supply the splenic flexure and distal third of transverse colon [26]. But in the present case the left branch of middle colic from celiac trunk supplied the splenic flexure and the proximal descending colon in the absence of middle colic artery from superior mesenteric artery and left colic artery from the inferior mesenteric artery. This is not mentioned in the literature (Fig. 7).
Left gastric artery is the smallest branch of the celiac trunk, enters the lesser omentum after turning anterioinferiorly at the upper end of the lesser curvature. It is the main artery supplying stomach and abdominal part of the oesophagus [26]. Mburu et al. [29], reported celiac trunk trifurcation in 61.7%, bifurcated in 17.9%, gave collateral branches in 20.3% out of 123 cases. Collaterals included dorsal pancreatic artery, gastroduodenal artery, inferior phrenic artery. Dorsal pancreatic artery is the most common collateral (14.8%) and inferior phrenic artery (4.9%) arising from celiac trunk [29]. Piao et al. [23] summarized the origin of inferior phrenic artery as: from aorta (61.6%), celiac trunk (28.2%), and left gastric (2.9%). In the present case left inferior pheric artery was arising from the celiac trunk.
Generally splenic artery shows a tortuous course. Tortuosity of splenic artery can be in the form of continuous irregular curves, one or more spirals, loops or twists, which usually lie in the groove on the upper dorsal surface of the pancreas, completely or partly covered by the pancreas [7]. In the present case splenic artery was completely covered by pancreas (retropancreatic) and highly tortuous with loops, which is very rare. Tortuosity mainly affects the pancreatic and prepancreatic segments of the splenic artery. Daisy Sahni et al. [30] found the splenic artery was tortuous only in 10% of adults. In the present case, splenic artery also gave an additional branch to distal third of transverse colon. Bamac et al. [31] reported a case of distal 1/3rd of the transverse colon supplied by a branch of splenic artery.
Coeliac trunk and superior mesenteric artery are two ventral branches of abdominal aorta which supply blood to wide area of supracolic compartment structures. The knowledge of variations in the origin of the hepatic arteries is very important during surgery like pancreaticoduodenectomy, liver transplant as well as during hepatic artery infusion chemotherapy. Preoperative imaging can help better preparation and planning by the surgical team. But all arterial variations may not be detected in preoperative imaging (only up to 60%–80% of cases) If detected it can help the surgeons to identify the artery and prevent its injury during surgery and post-operative complications like bleeding and ischemia [18]. Better understanding of the arterial supply to pancreas may lead to improved results in pancreas transplantation, regarding anomalous origin, size and course of the dorsal pancreatic artery as it plays a major role in the vascularization of the pancreas transplants [2425]. Knowledge of anamolous origin of middle colic artery is essential in cases of hemicolectomy and replacement of the oesophagus by the colon as they have recommended use of ascending branch of left colic for blood supply and the transverse colon for replacement of the oesophagus in an isoperistaltic fashion [32]. According to Lorenzini et al. [33], it is the left colic artery which they called as dominant artery supplies the splenic flexure. In case of absence of left colic artery, its place can be occupied by anomalous middle colic artery like in this case.
This study allowed to distinguish two very rare variations which, to my knowledge, have not reported before. Hepatomesenteric trunk with independent origin of left gastric and splenic arteries from abdominal aorta, left and right inferior phrenic arteries arising from them respectively. Middle colic artery arising from celiac trunk supplying splenic flexure of transverse colon and proximal descending colon.






 XML Download
XML Download