

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Since the first healthy child was conceived via intracytoplasmic sperm injection (ICSI) [1], this technique has become increasingly popular as producing viable embryos having high implantation potentials. In addition, in in-vitro fertilization, the operator attempts to select the morphologically best embryo to predict embryo viability as to guide selection of embryos for implantation.
In the Assisted Reproductive Techniques (ART) Laboratory, embryo formation influenced by extracellular morphological characteristics of oocyte, such as zona pellucida, polar body, cumulus oophorus, and intracellular properties have been related to fertilization, cleavage, embryo-formation, and clinical outcomes [2345].
Oocyte chromosomes at metaphase II (MII) stage are aligned at the equatorial region of the meiotic spindle (MS). This structure plays a vital role in the sequence of events leading up to the completion of meiosis and fertilization and thus is a key determinant of oocyte developmental potential. The MS microtubules, which are responsible for proper separation of chromosomes, are highly sensitive to physical and chemical changes that may occur during oocyte retrieval and handling. It has been shown that the oocyte exposure to slight temperature fluctuations dramatically affects microtubular structure, with deleterious consequences on chromosomal organization [678]. Other parameters, such as increasing maternal age [910] and oocyte in in vitro aging is associated with abnormalities in MS architecture [8]. The most potentially dramatic consequences of MS changes are unbalanced separation and/or non-separation of chromatids, chromosome scattering, and the formation of aneuploidy embryos [91112].
The MS, through the different stages of meiosis, controls chromosome movement, and is involved in various functions which are essential for fertilization and early postfertilization events. These include the accountability for proper chromosome segregation and genomic stability after oocyte activation [1314].
The zona pellucida is a unique extracellular coat that cinctures the maturing oocyte during ovulation, fertilization, and first embryo development [15]. A correlation between zona birefringence and the potential for an embryo to develop to the blastocyst stage has already been shown [1516].
Using the routine methods for observing the spindle, such as immunohistochemistry and electron microscopy are limited to fixed specimens. The key to improve the techniques of prediction of oocyte developmental potential may lie in advances in quantitative imaging of the MS. Development of a polarized light microscope which evaluates the birefringence of living cells enables the evaluation of oocyte spindles without damaging the cell, as spindles are highly birefringent [517]. In addition to the MS, polarized light microscopy enables the evaluation of other sub-cellular oocyte structures, such as zona pellucida birefringence [18]. In this study, we aim to evaluate the relationship between MS visualization, morphology and ICSI outcomes in human oocytes.
Materials and Methods
Patients
Twenty-four couples who were undergoing ICSI cycles at highly specialized Jihad Daneshgahi Infertility Treatment Center, Qom branch (ACECR Center for Infertility Treatment, Qom Branch) entered the study. Couples that were selected for this study met the following criteria:
Age under 38-years old, retrieval of at least 5 and at most 15 mature oocytes, absence of male factor and injection of oocytes 36–40 hours following human chorionic gonadotropin (hCG) administration.
Informed consents collection and grouping of patients
The trial design was approved by the Ethics Committee (registry No. 03-312) and all couples were required to sign a written consent before initiation of the treatment cycles.
Written informed consent was obtained from patients in which they agreed to share the outcomes of their own cycles for research purposes.
Patients divided into two groups: control microinjection group (polar body–aligned or PB-aligned) and treatment microinjection group (spindle-aligned). The control group has the oocyte aligned by the first polar body, a cell that separates from an oocyte during meiosis and contains a nucleus produced in meiotic division and very little cytoplasm, at the 6 or 12 o'clock position and the true location of the MS is unknown and sperm was injected at 3 o'clock. The MS of the spindle-aligned group was detected by polarized light microscope (CRI, Woburn, MA, USA) to align the spindle at 6 or 12 o'clock. Fertilization rate and embryo quality were compared between the oocyte groups. Our criteria was retrieving five mature oocytes, so patients with less than five mature oocytes were rulled out, since it was considered that there may not be a sensible chance of getting at least one embryo developing in each treatment group [19]. Surgically-retrieved-sperm patients undergoing ICSI was another factor of rulling out the patients.
Ovarian stimulation
Protocol of ovulation induction in all of the patients was standard long protocol. Pituitary desensitization with a gonadotropin-releasing hormone agonist and ovarian stimulation with gonadotropins (Merional, IBSA, Lugano, Switzerland), were carried out. The patient monitoring was done by transvaginal ultrasound and hCG was injected when at least three follicles more than 18 mm in diameter were seen in ultrasonography. Oocytes were recovered transvaginally under ultrasound guidance and ICSI was performed.
Preparation of sperm
Ejaculated spermatozoa were obtained by masturbation after 3–5 days of ejaculatory abstinence. After liquefaction of semen at room temperature, sperm samples were prepared by discontinuous density-gradient centrifugation. For discontinuous density-gradients, the bottom fraction was aspirated and washed with Quinn's sperm wash medium (ART-1006, SAGE BioPharma, Trumball, CT, USA) twice at 2,500 rpm for 4 minutes and incubated at 37℃.
Oocyte denudation
After retrieval, collected oocytes were incubated in culture medium (SAGE BioPharma) which was covered with mineral oil (Reproline, Rheinbach, Germany), at 37℃ and 6% CO2 for 3 hours. Cumulus cells were removed by 30-second exposure to 30 IU/ml hyaluronidase (SAGE BioPharma) in HEPES buffered human tubal fluid (HTF) followed by washing with HEPES-buffered HTF containing 5 mg/ml human serum albumin (SAGE BioPharma). The coronal cells were carefully removed by use of a series of finely drawn glass Pasteur pipettes [19]. Afterwards denuded oocytes were assessed for their structural integrity and meiotic maturity. The oocytes were randomized by using a random numbers table into the control and a treatment group and placed into fertilization medium (SAGE BioPharma) which was covered with mineral oil (Reproline), to await microinjection at 37℃ and 6% CO2.
Alignment method for spindle and microinjection
PB-aligned oocytes were transferred into 4 µl of warm HEPES buffered HTF containing 5 mg/ml human serum albumin (SAGE BioPharma), during microinjection and image analysis (Reproline). Sperm were placed in a 4 µl polyvinylpyrrolidone solution (LifeGlobal, Guilford, CT, USA) in the center of microinjection dish immediately before sperm injection; oocytes were placed under an inverted microscope (IX71, Olympus, Tokyo, Japan) with a heated stage at 37.0±0.5℃ and observed at ×400 magnification. Then the sperm was injected to the mature oocyte which its PB was in 12 or 6 o'clock position and then transferred to cleavage medium (SAGE BioPharma) and placed at 37℃ and 6% CO2. The PolScope optical (CRi'sPolScope Technology) requirements for the spindle-aligned oocytes (treatment group) necessitated a sterile, disposable, glass-bottomed dish (FluoroDish, Sarasota, FL, USA) to be used during spindle location and microinjection. The oocytes were classified as normal and abnormal spindle morphologically. Following microinjection and imaging, both oocyte groups were transferred to equilibrated individual 50 µl droplets for culture in cleavage media (SAGE BioPharma) in a sterile plastic dish in an incubator supplied with 6% CO2 at 37℃.
Temperature during oocyte and embryo manipulation was strictly maintained for all oocytes and embryos at 37℃.
Assessment of fertilization and embryo quality
Fertilization was assessed 16–20 hours after microinjection. All oocytes with an environmental chamber to maintain the temperature during imaging were returned to an inverted microscope [19].
Normally fertilized oocytes were returned to 50 µl individual cultural droplets of equilibrated cleavage medium (SAGE BioPharma). In order to check the presence of a 2-cell cleavage plane, embryos from the spindle aligned group were assessed 26–28-hour postmicroinjection [19]. If division had occurred, embryos were transferred to 4 ml HEPES droplets and aligned and re-imaged as above. Embryo morphology grading was performed 70±2 hours after microinjection when all embryos (control and treatment) were re-imaged. Embryo transfer was performed trans-cervically 2±3 hours later, utilizing a double catheter (COOK, Bloomington, IN, USA).
Alignment protocols images and definitions of early embryo development determining the morphology of embryos were obtained after microinjection on day 3 before transferring the embryo. This time allows evaluation of cleavage speed and embryo morphology and is considered a standard time for all embryos [19].
Following detecting the fragmentation percentage, morphology of the embryos were graded as: grade 1, spherical embryos with equal-sized blastomeres and no extra cellular fragmentation; grade 2, embryos with <10% fragmentation; grade 3, embryos with 30% fragmentation; and grade 4, embryos with >50% fragmentation. The number of zygotes showing pronucleus divided by the number of oocytes that survived the injection process was expressed as the fertilization rate for both groups, as oocytes can be abolished by the microinjection process and it's independent of the spindle presence [19].
Results
Oocyte and embryo parameters
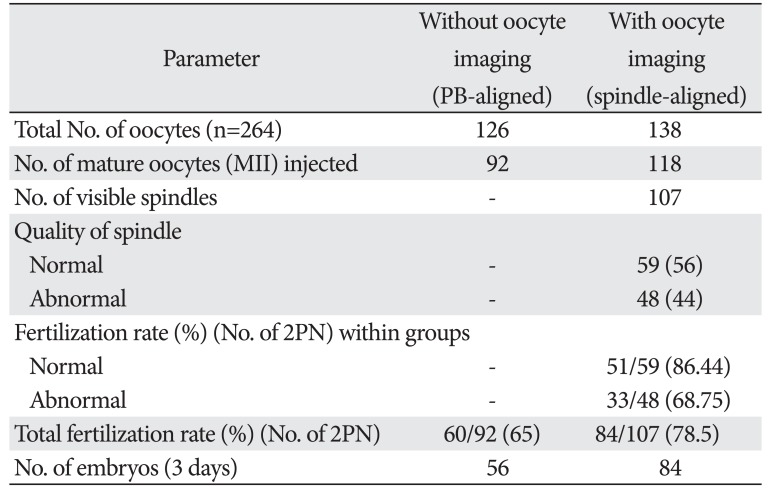
The oocytes of 24 patients were collected in this trial, with an average age of 30.5±7.5 years (range, 23–38 years), and a duration of infertility between 1 to 10 years. All the 264 oocytes were randomly allocated to the control injection group (n=126) and to the spindle injection group (n=138) (Table 1).
MS observation and morphology
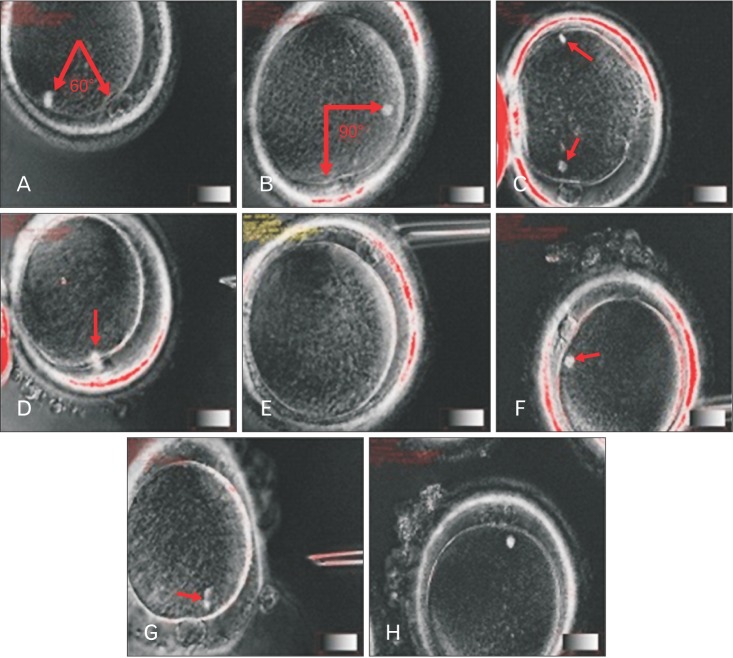
Out of the 138 oocytes allocated to the spindle-aligned group, 118 oocytes were MII (85%), 10 oocytes had no visible MS (7%), two oocyte had double spindle (2%) (Fig. 1C), and nine oocytes were in telophase stage (6%). There were 107 leaving oocytes (90%) with different visible spindle morphology at the time of microinjection. Different morphologies of visible spindle classified to normal 59/107 (55%) and abnormal 48/107 (45%) groups. Among these spindle-identified oocytes, 62.8% (67/107) of the first PBs were above the spindle or the lower region PB, and 6.9% (8/107) of the first PBs were in the opposite hemisphere to the spindle which is inserted into a poor group (Fig. 1).
Pronuclear assessment
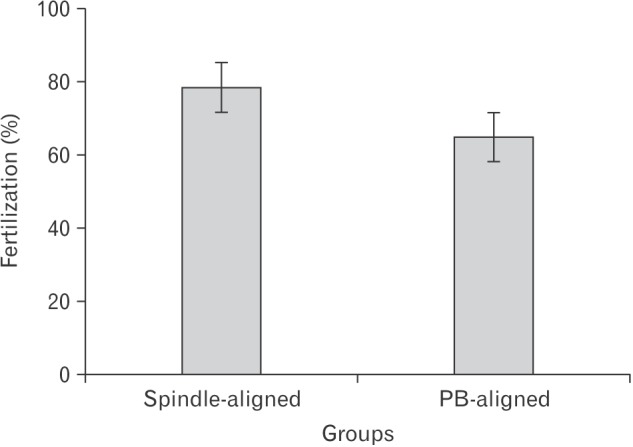
After 24 hours, embryos pronuclei (PN) were checked. The percentage of embryos with appropriate PN morphology was significantly higher among embryos derived from oocytes in which MS was viewed (78%) than among embryos derived from oocytes in which the MS was not checked (65%). In addition, fertilization rates were higher in normal MS morphology than others (Fig. 2). It should be noted that after ICSI in spindle-aligned group, the number of dead oocytes was reduced.
Embryo morphology scoring
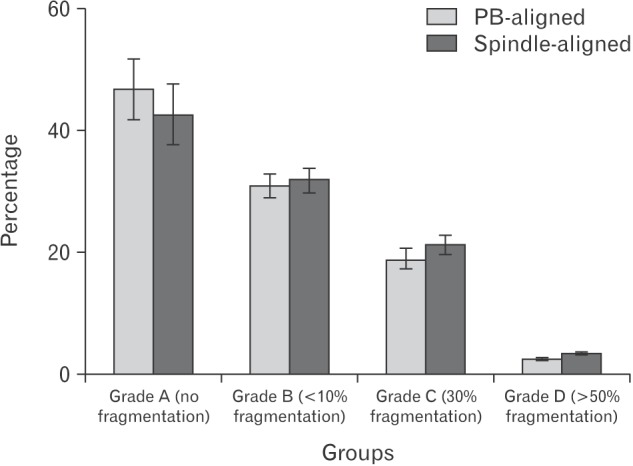
After 72 hours, morphology of embryos was checked and scored according to their quality. Embryos were divided into four groups 1–4. In spindle-aligned group, 47% (40/84) had grade 1, 31% (26/84) had grade 2, 19% (16/84) had grade 3, and 2.3% (2/84) had grade 4. In PB-aligned group, 42.8% (24/56) had grade A, 32% (18/56) had grade B, 21.4 (12/56) had grade C, and 3.5% (2/56) had grade D.
Discussion
The identification of predictive markers for oocyte developmental potential prior to fertilization is one of the most studied areas in assisted reproductive techniques. Up to now, a few predictive non-invasive markers for oocyte quality have been known on the basis of morphological criteria, which can be evaluated using conventional microscopy [20]. Our study indicated that the use of the polarization light microscopy is non-invasive, leading to reduced oocyte death after ICSI. Non-invasive imaging of the MS, enhances spindle quality, increases fertility and improves the quality of the embryos in comparison to the control group. Oldenbourg [21] mentioned that the introduction of polarization light microscopy enabled the non-invasive visualization of sub-cellular structures in oocytes such as the MS and zona pellucida birefringence.
Tomari et al. [22] and Keefe et al. [23] showed that polarization light microscopy for non-invasive imaging of the MS has become an important item in the laboratory to assess the competence of gametes.
Previous methods of imaging the MS, such as immunohistochemistry and electron microscopy were limited to clinical use. Since the polarization light microscopy is less sensitive than optical microscopes, it has been underused in embryology. Furthermore polarizing microscopes with higher safety for women undergoing ICSI treatment, help the thermodynamic stability of the egg during ICSI [23].
Polarized light microscope imaging helps to detect more oocytes and mature oocytes in MII in comparison to the control group. Also, this type of imaging helps to observe the spindle better. Assessment of MS normality is of a strong predictive value for pregnancy chances of a particular oocyte. Its true value in the selection of the “best” embryo for embryonic transfer needs to be confirmed by a randomized controlled study.
Those oocytes are more likely to result in an ongoing pregnancy. Evidence is mounting that the formation of the MS at 39–40.5 hours after exposure to increasing levels of luteinizing hormone (or its surrogate hCG) in MII oocytes is a sign of oocyte competency [24]. Presence of an MS has been associated with higher fertilization and pregnancy rates [1625]. In the MII stage oocyte, chromosomes are aligned in the center of the MS, which is involved in many functions that are essential for the sequence of events leading to meiosis completion and fertilization [14]. However, recent observations with more sensitive imaging capacity of the latest polarized light microscopy systems have shown spindles morphology and the uniformity of their birefringence. Therefore, categorization of the MS into normal spindle and abnormal spindle has become feasible. Abnormal spindles (Fig. 1F) have been associated with reduced fertilization rates. Several studies [1726] indicate the importance of presence of a detectable MS in the oocyte cytoplasm prior to ICSI. In this study, a clear positive correlation between MS visualization, fertilization rate, and/or embryo development was described. It should be noted that this method reduces the number of dead oocytes after ICSI. The absence of a recognizable MS and the consequent oocyte (Fig. 1E) developmental impairment may be primarily attributed to oocyte immaturity [812]. It has been hypothesized that the lack of MS formation can be the result of aberrant signaling pathways or low energy supply during oocyte growth, resulting in both nuclear and cytoplasmic immaturity [1227]. Moreover, some oocytes were found to be clearly immature at the stage of telophase I when observed with the spindle view system [81028]. At this stage there is continuity between the ooplasm and the cytoplasm of the forming first PB (Fig. 1G). Therefore, the spindle view system allows inaccurate determination of oocyte's nuclear maturity and selection of fully mature eggs is directly involved in the subsequent fertilization process. It is well documented that physical and chemical changes in the condition of the spindle can lead to failed or disrupted fertilization and subsequent development [7].
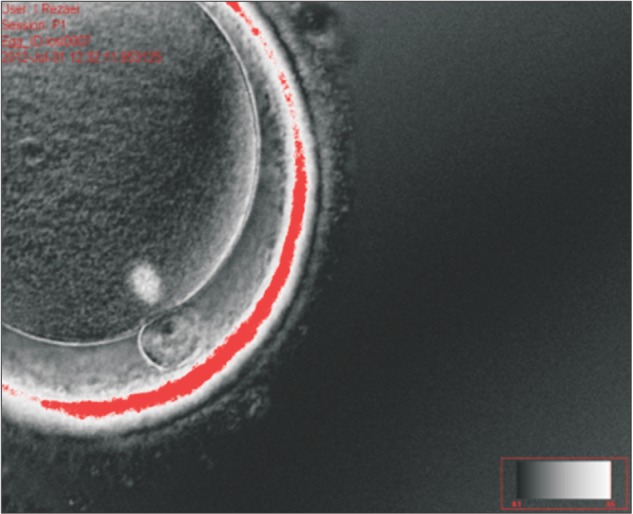
Long-term work with polarized light microscopy has resulted in the development of a definition of a “normal” spindle as having a barrel shape with clearly delineated boundaries and even distribution of birefringence (Fig. 4). These criteria can readily be used in the clinical setting with appropriate training of the embryologists.
De Sutter et al. [29] noted that the relationship between the morphology of oocytes and fertility success rate of ICSI program does not exist. Although some studies have demonstrated that morphologically normal oocytes are the most important factor in the production of high-grade embryos [30]. Furthermore, the results of Khalili et al. [31] showed that an oocyte with normal morphology not only significantly improves fertility rates, but also, with better production, ameliorates embryos in ART programs. This study indicates that imaging the MS morphology with a polarizing microscope can lead to better ICSI output in human oocytes. Furthermore, our results showed that spindle morphology and position of MS could predict fertilization rate and embryo morphology. In other studies, it is reported that close position of the MS to the PB was correlated with fertilization and cleavage rates and early embryo development and quality [19]. According to Rienzi et al. [28] high degrees of misalignment between the MS and the first PB increased risk of fertilization abnormalities. However, when normal fertilization occurred in such oocytes, the cleavage ability of developing embryos was not disturbed [28] and so Shen et al. [32] found that better pronuclear scores and higher pregnancy rates correlated with higher retardance [33]. However, in some researches, there was no significant correlation between the spindle retardance and embryo quality [34].
Polarized light microscopy, increases fertility and improves the quality of the embryos. It can improve the performance of laboratory and ICSI studies. Since fluorescent microscope can provide detailed information about chromosome and MS, further studies comparing polarizing and fluorescent microscope imaging methods seem necessary.
 XML Download
XML Download