

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The shape and volume of the alveolar process is determined by the presence or absence of the teeth, their form, and their direction and axis of eruption. When teeth are lost or extracted, a physiological process of remodelling of hard and soft tissues results in a dimensional shrinkage of the alveolar ridge in both height and width, depending on multiple variables including the alveolar socket size, the thickness of the mucosa, metabolic factors, and functional loading. A recent systematic review analysing dimensional changes of the alveolar ridge reported horizontal bone loss ranging from 29% to 63% and vertical bone loss ranging from 11% to 22% at 6 months after tooth extraction [1]. The resorption pattern is characterised by rapid reduction in the first 3–6 months, followed by gradual reduction thereafter [2]. Further, horizontal buccal bone resorption has been shown to reach as much as 56%, while lingual bone resorption has been reported to be up to 30% [3]. Major bone resorption of the vestibular wall of the extraction socket is related to a higher proportion of bundle bone, a tooth-dependent tissue through which the periodontal ligament fibres are anchored to the jaws, which undergoes resorption due to the loss of its function.
The volume reduction of the alveolar process may prevent or render difficult implant installation in a prosthetically driven position, simultaneously jeopardising the functional and aesthetic outcomes. Thus, ridge preservation treatment protocols have been developed in order to maintain the alveolar bone volume existing at the time of tooth extraction, and to ensure the support of an adequate ridge profile. Alveolar socket preservation (ASP) is a procedure in which a graft material is placed in the socket of the extracted tooth at the time of extraction, with or without the application of barrier membranes or soft tissue coverage, to preserve or improve the original ridge dimensions and to allow an ideal implant location.
A number of biomaterials for socket grafting have been reported, including autogenous, allogeneic, xenogeneic, and alloplastic bone grafts and other materials such as platelet-rich plasma, platelet-rich fibrin, bone morphogenetic protein, Emdogain, and cell therapy [4]. It was recently observed that after flapless extraction of teeth, using a minimum healing period of 12 weeks as a temporal measure, xenografts and allografts resulted in less loss of socket dimensions than alloplasts or sockets with no grafting [5]. Several preclinical and clinical studies have widely described the biocompatibility and the integration of deproteinised bovine bone mineral (DBBM) into the newly formed bone when used in the extraction sockets [67]. DBBM is a defatted and deproteinised xenograft reduced to porous grains of different dimensions (0.25–2 mm) and deprived of all its organic components through high-temperature processes in order to minimize the immune response [8]. A histological human study designed to determine the composition of tissues that formed after 6 months of healing in extraction sites grafted with DBBM confirmed that placement of the biomaterial in fresh extraction sockets delayed healing, but allowed preservation of the edentulous ridge [9], which in turn led to a significantly reduced dimensional loss when grafted vs. ungrafted sites were compared [10]. The ability to prevent dimensional changes in grafted sockets depends on the properties of DBBM particles, which can still be observed in the edentulous site even 7 months after the grafting procedure [11]. Nevertheless, post-extractive sockets grafted with DBBM showed a clinically sufficient quality and quantity of bone, allowing for correct implant placement after 9 months of healing [12].
Soft tissue management of the edentulous socket is another important factor for maintaining an optimal contour of the implant-supported restoration, along with biological and functional demands. It is generally accepted that flap elevation has a detrimental impact in bone remodelling because of the interruption of the periosteal vascular supply and an increase in post-surgical local inflammation. In addition, the use of a palatal soft tissue graft to seal the socket is associated with several disadvantages, including the need for a secondary site to obtain the tissue, risk of graft necrosis and subsequent clinical fibrous healing, increased operative time and patient morbidity [13]. From a practical and patient-centred standpoint, the use of xenogeneic collagen matrices led to promising results in terms of hard and soft tissue width and volume preservation [14]. Recently, a new xenogeneic, porcine non-cross-linked bilayered resorbable collagen matrix (CM) consisting of pure type I and III collagen was introduced for soft tissue regeneration [15]. The compact layer facing the oral cavity consists of compact collagen to fulfil the cell occlusive properties and allow tissue adherence and marginal adaptation as a prerequisite for favourable wound healing. In addition, the elastic properties of the smooth texture accommodate suturing to the host mucosal margins. The second layer consists of a thick, porous, spongy structure to allow tissue integration. This roughened surface is placed next to the host tissue to facilitate organisation of the blood clot and to promote haemostasis and angiogenesis [16]. Clinical and histological results demonstrated revascularisation, re-epithelisation, and safe integration of the CM into the surrounding tissue without any signs of inflammation; the CM was associated with greater thickness and width of the keratinised mucosa and a better color match than spontaneous healing [171819]. Since the CM can act as a resorbable membrane promoting guided bone regeneration for at least 30 days, it has been used as a device for ASP procedures in association with a biomaterial, providing encouraging results in maintaining the soft tissues and minimising ridge resorption in all dimensions [1020].
Hence, the purpose of the present pilot study was threefold: 1) to clinically and radiographically assess the magnitude of socket dimensional changes in both width and height, 2) to clinically evaluate soft tissue healing, and 3) to analyse the histologic and histomorphometric aspects of the grafted sockets filled with DBBM covered with a porcine-derived CM.
MATERIALS AND METHODS
Study design
The present study was a clinical, radiological, and histological multicentre evaluation conducted at 3 different university dental clinics in Milan, Italy, between January 2014 and January 2015. The surgical procedures were performed by 3 clinicians (Carlo Maiorana, Tiziano Testori, and Raffaele Vinci) with an in-depth knowledge of ASP and implant placement procedures. Histological preparations were performed at the University of Freiburg Medical Centre. The study was approved by the local ethical committee and was conducted according to the principles articulated in the Helsinki Declaration of 1975 for biomedical research involving human subjects, as revised in 2000. All patients were informed about the nature of the study and gave their written consent.
Patient population
All subjects included in the present study were over 18 years of age, presented healthy local and systemic conditions, and required a single tooth extraction and subsequent replacement with an implant in the upper jaw between the second premolars. All extraction sites had adjacent teeth. The exclusion criteria were those commonly used for oral surgery procedures: immuno-suppressed or immuno-compromised patients, subjects presenting uncontrolled systemic diseases, pregnant or lactating subjects, the presence of active periodontal disease associated with poor oral hygiene and motivation, subjects addicted to alcohol or drugs, smoking >10 cigarettes per day, patients with psychiatric problems, and patients with an acute infection (abscess) or presence of pus in or close to the site intended for extraction. Prior to enrolment, all patients were asked to sign a specific informed consent form to document that they understood the scope and the methods of the study as well as the possible treatment alternatives. Patients who refused to sign the informed consent form were not admitted to the study. Before study initiation, all subjects underwent a rigorous oral hygiene regimen, including any periodontal treatment when it was indicated, in order to provide an oral environment more suitable to wound healing. A template was fabricated on the study model, to serve as a fixed reference guide indicating the centre of the grafting site during the tissue harvesting procedure.
Biomaterials
During the socket preservation procedure, a xenogeneic bone substitute was used to fill the post-extraction socket, in association with a soft tissue substitute to cover the defect. The xenogeneic bone substitute consisted of deproteinised collagen-coated bovine bone mineral (Bio-Oss®, Geistlich Pharma AG, Wolhusen, Switzerland) in the form of granules with a diameter ranging from 0.25 to 1 mm; the product was always hydrated with sterile physiological solution before being applied to the socket, according to the manufacturer's instructions. The soft tissue substitute consisted of a porcine-derived non-crosslinked bioabsorbable CM (Mucograft® Seal, Geistlich Pharma AG) consisting of pure type I and III collagens, with a diameter of 8 mm, handled and applied in a dry state, according to the manufacturer's instructions. The compact macro-structure of the matrix faced towards the oral cavity to favour soft tissue re-epithelialisation, whereas the spongy framework was placed towards the extraction socket in order to stabilise the blood clot and the graft, favouring bone regeneration.
Interventions
T0 (baseline)
One week prior to surgery, a dental hygiene appointment was scheduled and patients were instructed to use a 0.12% chlorhexidine oral rinse (Dentosan®, Recordati S.p.A., Milan, Italy) twice a day for 1 minute.
On the day of surgery, a film holder (Rinn® XCP, Dentsply, York, PA, USA) customised directly in the patient's mouth using auto-polymerising acrylic resin was made to reproduce the same position of the film each time relative to the teeth adjacent to the surgical site, thereby obtaining super-imposable dental radiographs at different intervals. A periapical radiograph of the involved tooth was then obtained with the long cone paralleling technique, in order to have a baseline radiological reference.
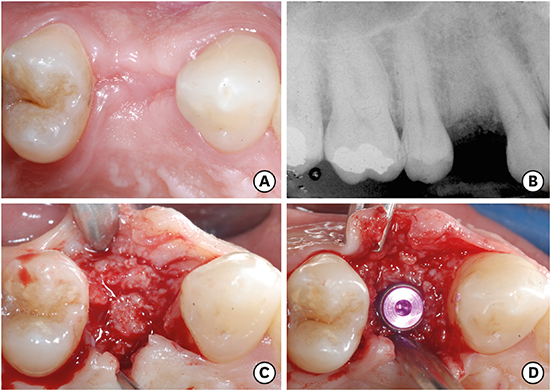
Surgical procedures were performed under local anaesthesia after administration of 2% carbocaine with 1:100,000 epinephrine (AstraZeneca S.p.A., Milan, Italy). A flapless minimally invasive tooth extraction was carried out in order to avoid any surgical trauma correlated to flap elevation and to decrease the reabsorption rate of the extraction socket (Figure 1A). Sindesmotomy was performed through intra-crevicular incisions performed with a sharp No. 15C surgical blade. An effort was made to preserve the interproximal papillae. Thin periotomes and appropriate dental forceps were used to minimise the surgical trauma to the surrounding tissues and to extract the tooth gently with slow rotational-pulling forces until the periodontal ligament fibres were torn completely. If necessary, multirooted teeth were sectioned to preserve all socket walls. After the tooth removal, the granulation tissue and the residual periodontal ligament fibres were curetted and removed by means of bone curettes. A probe was then used to verify the integrity of the extraction socket bone walls. Subsequently, a periapical radiograph of the edentulous site was conducted with the customised film holder, and intraoperative clinical measurements of the ridge dimensions were taken using a periodontal probe (PCP-UNC 15, Hu Friedy, Milan, Italy). In more detail, with the tip of the probe in contact with the most coronal bone tissue, the width of the alveolar ridge was measured in the bucco-oral dimension at the top of the crest using a small flap elevator to expose as little bone as possible at the midpoint of the extraction site, considering the distance between the most prominent sites on the buccal and oral side. Measurements were rounded to the nearest 0.5 mm. Following the technique of Landsberg [21], the epithelialised inner layer of the gingival walls at the socket orifice was removed gently by a sterile, water-cooled, high-speed, coarse, diamond bur to expose the vascularised lamina propria responsible for nourishing and revascularising the soft tissue graft to be placed at the socket orifice. The xenograft was then loosely packed to fill the socket until the coronal portion of the alveolar bone, avoiding excessive pressure in order to preserve the flimsy architecture of the scaffold itself (Figure 1B). Once the extraction socket was grafted, the bone graft was covered with a porcine CM that was trimmed and contoured according to the shape and dimension of the alveolar socket. The post-extraction socket was sealed with non-resorbable 6-0 simple interrupted suturing (Figure 1C). A peri-apical radiograph was conducted with the individualised film holder, serving as a post-operative radiological control (Figure 1D).
Figure 1
(A) Minimally invasive surgical extraction of the upper right first premolar with preservation of the vestibular and palatal cortical bone. (B) Demineralised bovine bone mineral grafted in the post-extraction alveolar socket. (C) Porcine-derived CM stabilised at the top of the alveolar socket with 6-0 non-resorbable interrupted sutures. (D) Peri-apical radiograph of the grafted socket performed immediately after the socket preservation procedure.
CM: collagen matrix.
The medications prescribed to all subjects consisted of 500 or 1,000 mg of amoxicillin (Augmentin, GlaxoSmithKline S.p.A., Verona, Italy) every 8 hours, based on the weight of the patient, for 6 days starting the day before surgery; 600 mg of ibuprofen (brand name, manufacturer, city, country) every 12 hours for 3 days, and 0.12% chlorhexidine oral rinse (Recordati S.p.A.), twice daily until suture removal starting 24 hours after surgery. Following surgery, patients were instructed not to brush the surgical site for 4 weeks, after which they resumed the use of a surgical (extra-soft) toothbrush in the surgical area for next 4 weeks, and then they started to brush regularly. Sutures were removed after 3 weeks.
Follow-up
Clinical evaluations of soft tissue healing and keratinized tissue replacement were assessed on the basis of the healing index proposed by Landry et al. [22] (Table 1). Recordings of healing index were performed on the first, second, fourth, eighth and, if not completely healed, on the 10th week post-surgery (Figure 2). The scores assessed healing on the basis of redness, presence of granulation tissue, bleeding, suppuration, and epithelisation. A score of 1 to 5 was given, with 1 associated with very poor healing and 5 being excellent.
Table 1
Soft tissue healing index according to Landry et al. [22]

Figure 2
(A) Healing of the soft tissues 1 week post-surgery. (B) Healing of the soft tissues 2 weeks post-surgery. (C) Suture removal 3 weeks post-surgery. (D) Healing of the soft tissues 4 weeks post-surgery. (E) Healing of the soft tissues 8 weeks post-surgery. (F) Healing of the soft tissues 10 weeks post-surgery.

T1
Six months after extraction, the re-entry procedure was performed in order to repeat the baseline radiological and clinical measurements, to collect hard and soft tissue biopsies, and to place implants (Figure 3A).
Figure 3
(A) Maturation of the soft tissues after a 6-month healing period. (B) Peri-apical radiograph of the grafted socket performed 6 months after the socket preservation procedure. (C) Maturation of the bone tissue 6 months after the ASP procedure. (D) Implant placed in the preserved socket in a prosthetically guided position.
ASP: alveolar socket preservation.
One week prior to surgery, a dental hygiene appointment was scheduled and patients were instructed to use a 0.12% chlorhexidine oral rinse (Recordati S.p.A.) twice a day for 1 minute.
The day of surgery, with the same customised film holder previously used to obtain the baseline radiological references, a peri-apical radiograph of the grafted socket was conducted, serving as a 6-month control reference (Figure 3B).
An antibiotic prophylaxis consisting of 2 g of amoxicillin clavulanate (GlaxoSmithKline S.p.A.) was administered 1 hour before surgery. After bacterial decontamination with a 0.2% chlorhexidine (Recordati S.p.A.) rinsing solution, local anaesthesia infiltration was performed with carbocaine 2% with epinephrine 1:100,000 (AstraZeneca S.p.A.). A circular operculectomy was performed with a 2.5-mm internal diameter trephine in order to harvest a soft tissue sample. To ensure correct positioning of the trephine, a surgical stent was fabricated on initial study casts indicating the centre of the extraction sites. Full-thickness flaps were then reflected to allow access to the alveolar ridges of the involved socket. The bucco-oral width of the alveolar ridge was re-evaluated at the midpoint of the alveolar crest with a periodontal probe (PCP-UNC 15, Hu Friedy) laid down at the bone crest limit. The template was again positioned to obtain a bone biopsy of the grafted site using another 2.5-mm internal diameter trephine (Figure 3C). Subsequently, the implant osteotomy was completed with a surgical handpiece and the implant was inserted (Figure 3D). First-intention free-tension healing was accomplished with 4-0 simple interrupted suturing (PROLENE®, Ethicon Inc., Somerville, NJ, USA).
A peri-apical radiograph was obtained with the individualised film holder, serving as a post-operative radiological control.
The post-operative medications consisted of 600 mg ibuprofen (manufacturer) every 12 hours for 3 days and a 0.2% chlorhexidine (Recordati S.p.A.) gluconate mouth rinse every 8 hours until suture removal, at 1 week.
Histologic and histomorphometric analysis
The tissue cylinders harvested during implant preparation were prepared for ground section according to methods described by Donath and Breuner [23]. In brief, bone biopsies were fixed in 4% formalin for 5–7 days, dehydrated in serial steps of ethanol (70%, 80%, 90%, and 100%), remaining for 1 day in each concentration, and cleared for 1 day in xylene (Merck KGaA, Darmstadt, Germany). Specimens were then infiltrated with Technovit 9100 VLC-resin (Heraeus Kulzer, Wehrheim, Germany) according to the manufacturer's instructions. After being embedded in the acrylic resin, the cylinders were polymerised and cut in the vertical plane in 500 µm sections using a precision cutting-grinding machine (Secotom-50, Struers, Ballerup, Denmark). The sections were mounted onto opacified acrylic slides (Maertin, Freiburg, Germany) and ground to a final thickness of approximately 60 µm on a rotating grinding plate (Struers). Specimens were subsequently stained with azure II and pararosaniline (Merck KGaA).
Following histologic preparation, the specimens were evaluated histomorphometrically by a single examiner masked to the study. All the specimens were digitalised at the same magnification using an Axio Imager M1 microscope equipped with a digital AxioCam HRc (Carl Zeiss, Göttingen, Germany). Histomorphometric analysis was performed under optical microscopy with image analysis software (analySIS® FIVE, Soft Imaging System, Münster, Germany). The following parameters were measured as percentages of the total sample area: the proportion of newly formed bone and residual graft material (stained dark magenta), the mineralised fraction, and the proportion of connective tissue and bone marrow (stained blue). For histomorphometric purposes, DBBM particles were digitally labelled green, while newly formed bone was labelled red. The measurements were expressed as percentages of the total sample area.
Radiological evaluation
For the radiographic assessments, the intraoral peri-apical radiographs taken immediately after alveolar ridge preservation and 6 months after the socket preservation were compared. The periapical radiographs were taken perpendicularly to the long axis of the alveolus with a long-cone parallel technique using the patient-specific customised film holder in order to increase the degree of reproducibility and to standardise the projection geometry between the pair of serially acquired images. Thereafter, the radiographs were scanned to obtain standardised digital images with a resolution of 1,200 dpi. These images were imported and superimposed using specialised computer software (ImageJ 1.49v, Research Services Branch, National Institute of Health, Bethesda, MD, USA). The calibration of the pixel/millimetre ratio was performed on the basis of a known distance (i.e., the length of the film), which was 41 mm in each radiograph. To calculate the apico-coronal dimension, the bottom of the socket was considered the most apical point, whereas the alveolar bone margin was considered the most coronal point of the socket bone wall.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS version 21.0, IBM Corp., Armonk, NY, USA). The recorded data were used for calculations of mean values and standard deviations (SDs). A post hoc analysis was performed to calculate the power of the study. The paired samples t-test was used to investigate the differences in terms of socket height and width between the pre- and post-operative examinations. The Friedman test with Bonferroni correction for multiple comparisons was run to determine if there was a difference with respect to the healing index score across weeks 1, 2, 4, 8, and 10. The cut-off for statistical significance was set at P<0.05.
RESULTS
Seven patients (4 females and 3 males; mean±SD of age, 49.1±6.2 years; range, 40–58 years) providing a total of 7 healing sites were included in the present study (Table 2). All treatments were performed according to the clinical protocol. All sites healed uneventfully with neither major complications nor dropouts. All patients completed the study and the 6-month follow-up. The quantity and quality of the newly formed bone allowed for prosthetically driven fixture insertion in all sites scheduled for implant treatment. The post hoc power analysis revealed a power of 93%.
Table 2
Distribution of sites across patients

Post-extraction dimensional changes of the ridge
Horizontal ridge changes are shown in Table 3. At baseline, the ASP sites had a mean initial bucco-palatal width of 9.35 mm, which decreased to 8.14 mm after 6 months of healing. A trend towards a reduced horizontal socket width was observed from baseline to the final examination. The resorption had a mean width of 1.21 mm (SD, 0.76 mm; 95% confidence interval [CI], 0.52–1.91 mm) and this difference was statistically significant (P=0.005).
Table 3
Horizontal dimensional changes of the sockets

Vertical ridge changes are shown in Table 4. As shown in the radiological evaluation, the ASP sites ranged from an initial alveolar mean height of 13.46 mm to 13.00 mm 6 months after the grafting procedure. A trend towards a reduced vertical socket height was observed from baseline to the final examination. The resorption had a mean height of 0.46 mm (SD, 0.27 mm; 95% CI, 0.21–0.71 mm) and this difference was statistically significant (P=0.004).
Table 4
Vertical dimensional changes of the sockets

Healing index evaluation
Recordings of the healing index (Table 5) indicated improvements in early wound healing. All sites showed the highest score after 10 weeks of healing. The index scores were significantly different through the time points (χ2=26.939; P<0.001) [4], with the following mean values: week 1, 2.0; week 2, 3.0; week 4, 3.9; week 8, 4.7; week 10, 5.0.
Table 5
Clinical evaluation of the soft tissue healing at the first, second, fourth, eighth, and tenth week after surgery

Histologic and histomorphometric evaluations
After a healing period of 6 months, hard and soft tissue biopsies were obtained from the grafted sockets. The evaluation of the sections stained with azure II and pararosaniline confirmed that all samples were healthy, without signs of inflammation, confirming the biocompatibility of both hard and soft tissue substitutes. With regard to the soft tissue, signs of mature submucosal and keratinised epithelial tissues were detected (Figure 4A). Dense, vascularised, collagen-rich connective tissue was recognisable in the coronal part of the specimens, indicating a proper substitution process of the CM (Figure 4B). In the most coronal part of some specimens, remnants of matrix material were found, as well as few granules surrounded by soft tissue (Figure 4C). More apically, DBBM particles appeared tightly integrated with newly formed bone trabeculae without fibrous encapsulation, confirming the process of osseointegration of the graft. In addition to the biomaterial particles, it was possible to identify the various biological elements forming bone tissue, including the traditional lamellar structure of the cortical mineralised bone, bone marrow spaces containing a collagen-rich connective matrix, and vascular structures (Figure 5A). The presence of active osteoblasts and seams of the osteoid matrix represented a clear sign of ongoing bone formation (Figure 5B).
Figure 4
(A) Microphotograph showing a biopsy of the mucosa after a 6-month healing period from a premolar site. Complete re-epithelialisation of the defect is visible, with biomaterial granules surrounded by an uninflamed area of connective tissue with coarse collagen fibres. Azure II/pararosaniline stain; bar=500 μm. (B) Higher magnification of the mucosa biopsy showed in Figure 4A, illustrating a multi-layered epithelium comprising the stratum basale, stratum spinosum, and stratum corneum, typical for the keratinised mucosa. Rete ridges and connective tissue papillae are well developed. Azure II/pararosaniline stain; bar=100 μm. (C) Higher magnification illustrating membrane remnants covered by mucosa epithelium and biomaterial granules surrounded by uninflamed connective tissue with coarse collagen fibres. Azure II/pararosaniline stain; bar=100 μm.
BO: biomaterial granules, E: epithelium, M: membrane remnants.

Figure 5
(A) Microphotograph illustrating biomaterial granules embedded in woven bone and in contact with well-vascularised, uninflamed, loose connective tissue. Biomaterials granules are connected via bony bridges. Azure II/pararosaniline stain; bar=100 μm. (B) Higher magnification of Figure 5A, illustrating seams of active osteoblasts forming dark-blue-stained osteoid. The biomaterial granule was in close contact with woven bone. No signs of acute inflammatory response were observed. Azure II/pararosaniline stain; bar=20 μm. (C) Microphotograph of the grafted site after 6 months of healing. The areas containing biomaterial show demineralised bovine bone granules in close contact with newly formed bone trabeculae. The loose connective tissue is well vascularised and free of inflammation. For histomorphometric purposes, biomaterial granules are labelled green and newly formed bone red. Azure II/pararosaniline stain; bar=500 μm.
BO: biomaterial granules, NB: new bone, OB: osteoblasts, O: osteoid.

The histomorphometric assessment was performed in specimens after 6 months of healing (Figure 5C). Data are presented as mean±SD. Newly formed bone made up 16.02%±7.06% (range, 6%–22%) of the examined tissues. Residual DBBM particles occupied 31.97%±3.52% (range, 27.1%–35.4%) of the area. The proportion of mineralised bone was 47.97%±6.77% (range, 38.1%–52.9%), whereas the amount of connective tissue and bone marrow was 50.67%±8.42% (range, 41.7%–61.9%).
DISCUSSION
The dimensional changes that occur in the alveolar ridge following tooth extraction have been evaluated using different methodologies, including clinical, radiographic, and cast model examinations, in addition to histological and histomorphometric analyses. Overall, it is well established that post-extraction sockets undergo vertical and horizontal bone loss, with the latter being proportionally greater. At the same time, socket intervention therapies might reduce post-extraction dimensional changes of the alveolus, but are unable to prevent resorption [24]. The present study investigated the dimensional changes and the histological healing of augmented extraction sockets within 6 months after tooth extraction. The sockets were grafted with DBBM and covered with a bioabsorbable porcine-derived CM. From the clinical and radiographic point of view, the residual ridge dimensions remained nearly stable, as highlighted by the mean height and width of bone resorption of 0.46 mm and 1.21 mm, respectively. This corresponds to a similar trial reporting that ASP with DBBM and bioabsorbable collagen membranes enabled the maintenance of most of the original ridge dimensions (92.74%) after a healing period of 4 months [25]. Accordingly, a recent retrospective analysis registered a volume loss of 9.9% when fresh sockets were grafted with DBBM covered by a resorbable collagen barrier and left to heal for 6 months [7]. The fact that after tooth extraction the horizontal bone loss was in general more pronounced than the vertical resorption has been clearly elucidated by several reviews [126]. As demonstrated by the present study, the same resorptive pattern also occurs in sockets preserved with DBBM. Our results compare favourably with a recent systematic review of randomised controlled trials reporting a mean loss of height from the ridge crest of 0.57 mm and a mean loss of bucco-lingual width at the crest level of 1.3 mm when xenografts were grafted into extraction sockets [5]. When the dimensional changes obtained in the present study were compared to non-grafted sockets, encouraging results emerged. It has been recently reported that post-extraction sockets underwent a horizontal dimensional reduction of 3.79±0.23 mm and vertical bone loss of 1.24±0.11 mm after 6 months of unassisted healing [1]. Thus, it can be assumed that ASP results in less horizontal and vertical ridge alterations with respect to non-grafted sockets. This finding was confirmed by a recent meta-analysis reporting that applying ASP techniques compared with unassisted socket healing could preserve approximately 1.31 mm to 1.54 mm of bucco-oral bone width and 0.95 mm to 1.12 mm of bone height, based on an analysis of studies with a follow-up of 6±1 months [27]. In particular, if compared to spontaneous healing, ASP by means of DBBM and CM showed significantly less reduction in ridge width (4.48±0.65 mm vs. 1.04±1.08 mm) and height (1.54±0.33 mm vs. 0.46±0.46 mm), respectively [25]. Comparable results were obtained in a similar trial, in which ASP was performed with a cortico-cancellous porcine bone xenograft covered by a soft cortical membrane. Extraction-only sites exhibited a significantly greater width of resorption of the alveolar ridge than the ASP sites (3.7±1.2 mm vs. 1.8±1.3 mm, respectively). Along with the bucco-lingual/palatal dimension, even the mean vertical ridge reduction was more pronounced in the control sockets with respect to the ASP sites (3.1±1.3 mm at the buccal sites and 2.4±1.6 mm at the lingual sites vs. 0.6±1.4 and 0.5±1.3 mm, respectively) [28]. Therefore, there is substantial evidence that the greatest loss happens in the horizontal plane of the residual alveolar ridge, which occurs along with vertical reabsorption that takes place primarily at the expense of the buccal aspect of the socket. In this regard, fresh extraction sockets filled with DBBM fared better in terms of buccal plate resorption than non-grafted sockets [29]. The management of the buccal bone plate plays a pivotal role when it comes to the aesthetic outcome of the implant therapy. Further, a facial bone thickness ≤1 mm corresponded to 69% of the maxillary central incisors and was associated with greater vertical bone loss than was observed in thick-wall phenotypes [30]. Thus, it would seem prudent to graft the socket with an osteoconductive biomaterial to reduce the loss of the buccal plate and the resulting drawbacks in implant treatment.
In addition to the maintenance of adequate bone volume, the generation of good tissue volume becomes essential to simplify implantation procedures and aesthetic outcomes. This can be accomplished with a primary wound closure by means of autogenous soft tissue grafts, barrier membranes, or soft tissue replacement matrices. In order to avoid patient morbidity related to the palatal donor site in case of soft tissue autografts, CMs of porcine origin have been developed as soft tissue substitutes. Such CMs, when used as a soft tissue substitute aiming to increase the width of keratinised gingiva, were as effective and predictable as the connective tissue graft, but their use was associated with a significantly lower patient morbidity [17]. Further, the use of CMs has been shown to accelerate wound healing compared to spontaneous healing as well as providing better color matching and less wound sensitivity [18]. These findings corroborate the results obtained in the present study with respect to the soft tissues healing index. Healing occurred without complications, and the exposed portions of the membranes were slowly replaced by mature keratinised tissue over 2 post-operative months. A score of 5 was given to all the extraction sockets after a healing period of 10 weeks. This might be explained by the ability of the CM to stabilise the blood coagulum and to serve as a scaffold to accelerate the migration of epithelial cells derived from the surrounding tissue, simultaneously maintaining the phenotypic characteristics of the recipient bed. In the present study, the re-epithelialisation of the graft was also promoted by de-epithelialising the soft tissue walls at the socket orifice to favour the nourishment and revascularisation of the CM [21]. As observed in a recent randomised controlled clinical trial, it might be suggested that the use of porcine CM as an adjunct to the ASP with DBBM may represent an alternative to the epithelial connective tissue graft by reducing surgical time and patient morbidity [31].
All the aforementioned clinical results have been validated by histological and histomorphometric analyses. The histological observations reflected the physiological healing pattern observed when fresh extraction sockets were filled with DBBM. Newly formed bone surrounding particles of the biomaterial was detected in most parts of the extraction site. As noted by Araújo et al. [6], osteoblasts that laid down bone mineral in the collagen bundles of the provisional matrix were clearly visible, representing de novo bone formation and hard tissue integration of the biomaterial. Apparently, the healing of the socket with respect to bone formation was faster in the apical and lateral portions than in more central and marginal regions. In fact, as reported by Carmagnola et al. [12], a histological examination revealed that the central portion of the augmented bone was mainly occupied by DBBM particles. In the present study, the proportions of newly formed bone and connective tissue were 16.02%±7.06% and 50.67%±8.42%, respectively. This agrees with previously reported findings and might indicate that that the use of biomaterial as fillers in extraction sockets may delay tissue modelling and remodelling [12]. Further, there are reasons to assume that with longer healing time, the amount of DBBM associated with new bone formation may increase [9]. This was supported by Hallman et al. [32], who found that after grafting the sinus with a mixture of autogenous bone and xenograft, tissues sampled after 6 months included about 20% of lamellar bone, while at 3 years, lamellar bone made up 51% of the harvested tissue. Similarly, Sartori et al. [33] followed up the rate of DBBM resorption with histomorphometric analyses at 8 months (29.8% newly formed bone and 70.2% DBBM), 2 years (69.7% newly formed bone), and 10 years (86.7% newly formed bone), underlying the slow metabolisation of DBBM by osteoclasts, as confirmed by the progressive increase in relative bone volume. In contrast, recent evidence has highlighted the absence of statistically significant differences between various ASPs and control sites in terms of bone formation and connective tissue percentages, even considering different follow-up times [34]. The fact that ASPs seem to resemble the physiological healing process in extraction sockets without improving the histological modifications in treated sites might lead to earlier implant placement, such as just 3 or 4 months after tooth extraction.
According to Cardaropoli et al. [25], ASP enabled the maintenance of most of the original ridge dimensions and allowed implant placement without the need for bone augmentation. This may have been related to the use of a graft material with a low resorption rate, enabling the maintenance of the grafted site and promoting hard tissue formation by acting as a scaffold with osteoconductive characteristics. This was corroborated by the percentage of residual DBBM particles, which occupied 31.97%±3.52% of the area. This indicates that particles of bovine bone mineral may not be resorbed at socket sites, but instead may remain more or less unaltered. The validity of this hypothesis is further supported by other studies that reported a similar proportion of biomaterial in grafted sites at 6 months and at 3 years [3235]. Additional validation of this finding comes from a recent systematic review reporting that after ASP, xenografts and alloplasts showed higher percentages of residual graft material than allografts (37.14% and 37.23% vs. 12.4%–21.11%, respectively) [34].
The use of a CM intentionally left exposed to the oral cavity converted the socket into a self-contained 4-wall defect. This may have increased the potential to maintain the socket volume, preventing soft tissue ingrowth during the early phase of wound healing. Interestingly, in the most coronal part of some specimens, few granules of biomaterial surrounded by soft tissue have been observed clinically and histologically. This might be explained by the rapid resorption of the CM during the first 2 weeks of healing. A similar resorption pattern was also observed in an experimental animal study, in which the CM left exposed to the oral cavity almost disappeared after 2 weeks [36]. This behaviour related to premature loss of the collagen or to rapid resorption, allowing fast re-epithelialisation of the oral mucosa, remains poorly understood. Conversely, other studies have pointed out the ability of the CM to maintain its barrier function for at least 30 days [151719]; however, this could not be confirmed in the present study. In any case, a more favourable outcome was reported for sites treated with a socket seal than for sockets left to heal spontaneously [37]. Our results compare favourably with another similar study reporting that a membrane-protected grafted socket showed more newly formed bone than unprotected grafted sites [38]. Covering the socket with a membrane confined the grafted particles during the first period of healing and stabilised the blood clot, unlike at unprotected sites. Emerging data suggest that keeping the biomaterial stable and separated from the oral cavity might provide long-term stability of soft tissues after ASP regardless of the type of sealing agent [39].
In conclusion, the application of DBBM particles covered with a CM to fresh extraction sockets allowed the preservation of an adequate hard and soft tissue volume to place implants, without the need for further augmentation procedures 6 months after tooth extraction. From a histological standpoint, the xenograft particles were partially resorbed and surrounded by newly formed bone, supporting the effectiveness of this material in promoting socket preservation. The CM demonstrated clinical efficacy for creating sufficient width and thickness of newly formed keratinised tissue, even if left exposed.
 XML Download
XML Download