

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Previous studies have shown that the clinical appearance of periodontal tissue differs among individuals [1]. Such variations in morphology have been referred to as the gingival biotype [2], and periodontal biotypes have been suggested to influence the results of restorative treatments [3]. Specifically, the thick gingival biotype has been reported as a prognostic factor for aesthetically successful outcomes of periodontal treatment [45]. However, patients with a thin gingiva are at higher risk for gingival recession after the placement of immediate implants [3] and less root coverage after periodontal surgery [6]. Gingival thickness and underlying alveolar bone thickness in the aesthetic zone seem to play a decisive role in treatment outcomes. Some studies have reported a moderate correlation between soft tissue thickness and the thickness of the underlying hard tissue [78]. However, due to the lack of standardized techniques for measuring hard and soft tissue thickness at identical positions, relatively few studies addressing this issue have been conducted. The most commonly used methods to measure alveolar bone thickness are calipers [9] and cone-beam computed tomography (CBCT) scans [1011]. In studies using CBCT scans, clear distinctions have been reported among subjects and tooth types.
Several methods have been proposed for assessing soft tissue thickness. The simplest method is based on the visibility of the periodontal probe outline through the soft tissue while probing the buccal gingival sulcus [12]. If the outline of the probe can be detected visually, the biotype is classified as thin; if not, it is classified as thick. However, conflicting results have been reported regarding the accuracy of this method [81314]. Another transgingival probing method utilizes endodontic needles and has been suggested as a way to measure soft tissue thickness directly [1516]. However, this method is invasive and requires the obtained values to be rounded. Alternatively, ultrasonic devices have been proposed to measure gingival thickness [17]. Although such ultrasonic methods are noninvasive and exhibit good reliability, their ability to accurately determine the thickness of a specific site is limited. Recently, digital scanning and assessment methods have been applied to measure the volume of periodontal tissues. This approach has been successfully used to assess volumetric changes in soft and hard tissues in clinical studies [18]. Indeed, studies have demonstrated the precision and reliability of this noninvasive method [19], although the possibility of introducing errors with the impression-model fabrication procedure has also been described. Several reports have measured soft tissue dimensions and hard tissue thickness using CBCT images [720]; however, more accurate outlines could be obtained through digital scanning files, with substantially higher resolution.
The limitations associated with the above methods of studying the relationship between soft and hard tissue thickness, such as their invasive nature and their limited accuracy, warrant further studies in this area, in addition to the development of superior methodologies. Based on the direct intraoral scanning and superimposing method, we can limit the incidence of errors that occur during the impression procedure. Thus, the aim of this study was to measure buccal bone thickness and gingival thickness using a noninvasive and relatively accurate digital registration method.
MATERIALS AND METHODS
Patient selection
Among patients who visited the Department of Periodontology, Seoul National University Gwanak Dental Hospital for annual scaling between October 2015 and June 2016, 21 patients 20–65 years of age in whom all maxillary front teeth (#11, 12, 13, 21, 22, and 23) showed no signs of marginal or periapical bone loss were included. The following exclusion criteria were applied: 1) pregnant women; 2) patients with fixed partial dentures or orthodontic appliances; 3) patients with systemic disease or who were taking medication that may have affected soft tissue thickness, such as calcium channel blockers or immunosuppressive drugs; and 4) patients with signs of either periodontal disease, defined as a periodontal probing depth >3 mm, or gingival recession.
After excluding 1 subject due to deficiencies in the quality of their radiographic images, a total of 20 participants (10 male and 10 female) were included in this study. Each participant provided written informed consent after being presented with a thorough explanation of the nature, risks, and benefits of this clinical investigation. The study protocol was approved by the Ethics Committee of Seoul National University, and the investigation was carried out in the Department of Periodontology, Seoul National University Gwanak Dental Hospital (EC/S-D20150029).
Stereolithography (STL) image acquisition and data matching
All subjects received scaling followed by the attachment of 3 radiopaque cylindrical fiducial markers on both maxillary second premolars and 1 incisor. After obtaining a CBCT scan (CS9300, Carestream, Rochester, NY, USA) of the maxilla, the maxillary arch of each participant was optically scanned with a 3-dimensional intraoral scanner (Trios, 3Shape, Copenhagen, Denmark). The 3 fiducial markers were used as a reference to match the scanned STL files with the CBCT images. Image reconstruction for visual analysis was performed using the Platon software (Ezplant, Seoul, Korea) to automatically superimpose the images using a series of mathematical algorithms.
Image analysis and measurements
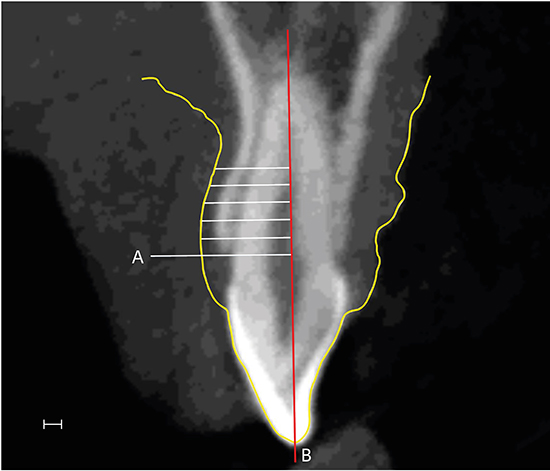
First, 1 of the 2 corresponding teeth in the first and second quadrants was randomly selected from the superimposed images. A longitudinal slice that divided the crown mesiodistally into 2 equal parts was then selected. A line coinciding with the axis of the tooth was then drawn in the transversal images of the sections.
Measurements of buccal bone thickness and gingival thickness were performed to the nearest 0.01 mm, 1–5 mm from the alveolar crest (A) at the mid-buccal aspect of each single rooted tooth and (B) perpendicular to the axis of the tooth. The gingival thickness at the alveolar crest line (G0) was also determined (Figure 1). All sites were measured by the same clinician. To assess intra-examiner reliability, duplicate registration was performed.
Statistical analysis
Data were analyzed using the R statistical software package (Version 3.3.1, R Foundation for Statistical Computing, Vienna, Austria), and the level of significance was set at 0.05. The Friedman test was used to compare buccal bone and gingival thicknesses for each depth between the 3 tooth types (central incisors, lateral incisors, and canines). If a significant difference was observed, tooth types were compared in a 2-by-2 manner using the Nemenyi post-hoc test. The Spearman correlation coefficient was calculated to assess the correlation between buccal bone thickness and gingival thickness at each depth according to the tooth type.
RESULTS
Mean thickness of hard and soft tissues at each level
Buccal bone and gingival thicknesses were measured 1–5 mm from the alveolar crest. Based on the mean values at each level, a tendency emerged for gingival thickness to increase and for bone thickness to decrease toward the root apex (Table 1, Figure 2). The mean buccal bone thickness at the central incisors, lateral incisors, and canines was 0.86, 0.83, and 0.90 mm, respectively. The mean gingival thickness at the central incisors, lateral incisors, and canines was 0.92, 0.83, and 0.81 mm, respectively.
Table 1
Mean thickness of hard and soft tissues at each level

Frequency distribution of buccal bone and gingival thickness
A frequency distribution according to tooth type and point of measurement is shown in Figure 3. For the central incisors, 77 sites had a buccal thickness of 0.5–1.0 mm, and 23 sites had a thickness of 1.0–1.5 mm. No sites had a thickness greater than 1.5 mm or less than 0.5 mm. At the lateral incisors, 61 sites were 0.5–1.0 mm thick, and 25 sites were 1.0–1.5 mm thick. A total of 10 sites had a thickness less than 0.5 mm, while only 4 sites exhibited a thickness of 1.5 mm or more. For the canines, 63 sites were less than 1.0 mm thick, 37 sites were 1.0–1.5 mm thick, and no sites more than 1.5 mm thick were detected. For gingival thickness, the proportion of sites less than 1.0 mm thick was 88%, 82%, and 91% at the central incisors, lateral incisors, and canines, respectively.
Figure 3
Frequency distribution of buccal bone and gingival thickness per point of measurement. (A) Frequency of buccal bone thickness at central incisors; (B) Frequency of buccal bone thickness at lateral incisors; (C) Frequency of buccal bone thickness at canines; (D) Frequency of gingival thickness at central incisors; (E) Frequency of gingival thickness at lateral incisors; and (F) Frequency of gingival thickness at canines.

Comparison of buccal bone and gingival thickness with respect to tooth type
According to the results of the Friedman test, a significant difference was found among tooth types for G0 (P=0.004), gingival thickness 1 mm inferior to the alveolar crest (G1) (P=0.025) and buccal bone thickness 5 mm inferior to the alveolar crest (A5) (P=0.025). The post-hoc tests indicated a significant difference in G0 between the central incisors and canines (P=0.032) and between the central incisors and lateral incisors (P=0.013). At the G1 level, a difference was found between the central incisors and canines (P=0.025). Finally, for buccal bone thickness 5 mm under the alveolar crest, the lateral incisors and canines were significantly different (P=0.025) (Table 1, Figure 4).
Figure 4
Comparison between buccal bone and gingival thicknesses according to tooth types. There was a significant difference among tooth types for G0, G1, and A5.
CI, central incisor; LI, lateral incisor; CA, canine; G0, gingival thickness at alveolar crest line; G1, gingival thickness at 1 mm inferior to the alveolar crest; A5, buccal bone thickness at 5 mm inferior to the alveolar crest.
a)Statistically significant difference (P<0.05).

Relationship between buccal bone and gingival thickness
The results of the Spearman correlation tests are shown in Table 2. No correlation between buccal bone thickness and gingival thickness was found at any depth level according to tooth type.
Table 2
Spearman correlation values between buccal bone thickness and soft tissue thickness at each level according to tooth type
DISCUSSION
Accurate measurements of the soft and hard tissue dimensions are important because they affect the outcomes of periodontal treatment, particularly in aesthetically critical areas. Therefore, the maxillary anterior regions have frequently been analyzed, with the goal of developing reliable guidelines for the identification of critical cases with thin gingiva and/or alveolar bone [111620]. This report describes a novel technique utilizing superimposed CBCT images and optically scanned files that consistently produced images that allowed soft and hard tissue dimensions to be measured at identical levels. We used a radiopaque marker attachment technique to improve the accuracy of image matching. Using this simple and noninvasive technique, it was possible to reconstruct precise para-axial images of teeth, including the buccal bone and gingival contour. Compared with other recent studies [1718], this method was associated with a smaller possibility of errors resulting from impression procedures and the use of bulky ultrasonic instruments. In addition, the method described here was also able to measure bone and gingival thicknesses at identical levels and at various depths.
According to our results, the buccal bone thickness at the central incisors, lateral incisors, and canines was 0.86, 0.83, and 0.90 mm, respectively. Overall, the percentage of sites with a thin buccal wall (<1 mm) was notably high: 77% at the central incisors, 71% at the lateral incisors, and 63% at the canines. Several studies have measured bone thickness using CBCT. Younes et al. [17] reported mean values of 1.07, 1.16, and 0.98 mm at the same sites, respectively. In other studies, the buccal bone of the maxillary frontal teeth was relatively thin [11]. One possible explanation for the relatively thin bone observed in our study is a race-related aspect of bony architecture [17]. Consistent with this possibility, a previous study performed in Korea reported that the buccal bone was extremely thin [10]. This discrepancy could also be the result of a difference in CBCT settings or software inaccuracies during the measurement of bone thickness. In the present study, no cases of thick buccal bone walls (≥2 mm) were identified, similar to the results reported by Younes et al. [17] and Nowzari et al. [21]. Since most tooth sites in the anterior maxilla have a thin facial bone wall, they may undergo marked dimensional diminution following tooth extraction.
The mean gingival thickness at the central incisors, lateral incisors, and canines was 0.92, 0.83, and 0.81 mm, respectively, which are generally thinner than the values reported in the literature [1622]. In those studies, gingival thicknesses showed a decreasing tendency from central incisor to lateral incisor and canine as well as the results of this study. Interestingly, the results for mean thickness at each depth level exhibited a similar tendency for the central incisors, lateral incisors, and canines. Specifically, the mean values of gingival thickness increased and bone thickness decreased toward the root apex. The lack of accuracy in measurements of gingival thickness under the mucogingival junction due to mobility of the gingiva may have influenced this result.
We also examined the relationship between buccal bone thickness and soft tissue thickness. To predict the outcomes of periodontal treatments by detecting gingival thickness alone, it may be important to investigate the correlation between soft and hard tissue thickness. A perfect match of the hard and soft tissue registration area is necessary to perform such an analysis, which was achieved in this study using a digital superimposition method. However, this approach did not reveal a significant correlation between hard and soft tissue thickness at any depth level, in contrast to previous findings. Specifically, Stein et al. [8] performed a comparative study of 60 subjects and reported a positive correlation between buccal bone thickness and gingival thickness. However, the comparison in their study was not carried out at an identical level. Instead, gingival thickness was evaluated at the supracrestal level, while bone thickness was measured under the alveolar crest. In contrast, in an in vivo study of 90 maxillary teeth, La Rocca et al. [16] observed no significant correlation between the results of CBCT scans and transgingival probing, although the comparison in their study was also not performed at an identical level. Considering these conflicting results, and despite the limited sample size of our study, we believe that our results suggest that gingival thickness is not associated with the thickness of the underlying bone.
Comparisons among tooth types have been made in several studies [1117], due to the difference of tooth angulation and convexity of the root shape between the central incisors, lateral incisors, and canines. In contrast to the lack of correlation between hard and soft tissue thicknesses, we observed a significant difference in thickness among tooth types at G0, G1, and A5. Specifically, proximity to the alveolar crest level (G0, G1) was associated with a significant difference in gingival thickness between the central incisors and canines. In contrast, buccal bone thickness was only different at A5, close to the root apex, between the lateral incisors and canines.
In conclusion, despite morphologic variations of the periodontium, the gingival and buccal bone thicknesses of anterior maxillary teeth were found to be relatively thin (<1 mm) overall. A tendency emerged for gingival thickness to increase and bone thickness to decrease toward the root apex. Finally, a difference was found between teeth at some positions, although the correlation between buccal bone thickness and soft tissue thickness was generally not significant.
 XML Download
XML Download