

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Peritoneal dialysis (PD)-related peritonitis is common in end-stage renal disease patients on continuous ambulatory peritoneal dialysis, with an incidence of 0.06–1.66/patients/year1), and can cause peritoneal injury and cessation of PD2). Most cases of peritonitis are caused by penetration of bacteria into the lumen or through the peritoneal catheter tract3).
The most frequent cause of peritonitis is Staphylococcus epidermidis, which is found in skin; however, several Gram-negative bacteria including Pseudomonas can be the causative organisms4). We report a case of automated PD-related peritonitis caused by Aeromonas hydrophila, which has only been reported in less than 10 cases worldwide.
Case Report
A 56-year-old male had been on automated PD for 6 months. The cause of his end-stage renal disease was diabetes mellitus and his PD regimen involved 4 cycles of 2-L exchanges using 1.5% solution over 7 hours, with intervening dry days. He was admitted to our hospital because of acute abdominal pain and cloudy dialysate since the day before admission. He admitted that he had recycled the sleep-safe Set Plus (Fresenius Medical Care, Germany), a disposable component of the automated PD device, by washing with tap water. On admission, he had diffuse abdominal tenderness and a clear exit site. His vital signs were as follows: blood pressure, 99/56mmHg; heart rate, 97/min; body temperature, 36.8℃; and respiratory rate, 20/min.
The total dialysate leukocyte count was 121,157/mm3, with neutrophil predominance of 89%. The hemoglobin level was 9.7 g/dL, The white blood cell (WBC) count was 13,450/mm3 (neutrophils, 89.1%; lymphocytes, 5.7%; monocytes, 4.9%), and C-reactive protein level was 16.50 mg/L. Peritoneal effluent and blood cultures were obtained before administration of antibiotics. The patient's regimen was changed from nocturnal intermittent PD to continuous ambulatory PD and he empirically received intraperitoneal vancomycin 1.5 g every 4 days and ceftazidime 1 g/day.
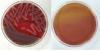
His symptoms were much improved, and the serum and dialysate leukocyte counts were markedly reduced after administration of antibiotics (Fig. 1). The peritoneal effluent stained positive for Gram-negative rods. A. hydrophila initially grew out in a blood culture bottle of the peritoneal dialysate, and was then cultured on blood agar and MacConkey agar plates (Fig. 2); however, the blood culture was negative. A. hydrophila was also identified using matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS, BIOTYPER 2.0; Bruker Daltonics, Bremen, Germany). The organism had confirmed susceptibility to ceftazidime and ciprofloxacin (Vitek-II AST-N224 card; bioMerieux, Marcy l'Etoile, France). Based on the culture and sensitivity results, vancomycin was discontinued and only ceftazidime was continued for 21 days. The dialysate WBC count decreased to 1,000/mm3 after 3 days, finally falling to 10/mm3. The patient was successfully treated without PD catheter removal and was discharged on day 8. After discharge, he remained well without recurrence of PD-related peritonitis at 1-year follow-up.
Discussion
Peritonitis remains a major complication of PD, accounting for much of the technique failure and high mortality in PD patients. A breakdown in aseptic technique can lead to peritonitis and many patients on PD are presumed to be inadequately educated on the care of their PD equipment. The most common source of peritonitis is contamination owing to technique failure at the time of exchange. Technique failure accounted for about 21% of peritonitis episodes5).
This is apparently the second reported case of PD-related peritonitis caused by A. hydrophila in Korea6). The cause may have been reuse of a disposable Set Plus rinsed with tap water, which could lead to penetration of A. hydrophila through the abdomen. We treated the patient with intraperitoneal vancomycin and ceftazidime and he has remained well without recurrence for 2 years.
A. hydrophila is a Gram-negative rod that can live in aerobic and anaerobic environments. Aeromonas species are widely found in the environment and have been isolated from water, soil, food, and even human feces7). A. hydrophila mainly causes infections in freshwater fish and amphibians.
A. hydrophila infections are common in patients with preexisting viral or other bacterial infections, and can be triggered by stress and changes in surroundings and temperature8). The route of infection is ingestion of contaminated meat, seafood, and even vegetables.
A. hydrophila can cause infection in children and immunocompromised patients.
A. hydrophila can cause cellulitis, acute diarrheal disease, sepsis, and other infections910). High mortality rates have been reported in cases of bacteremia and peritonitis caused by Aeromonas in immunocompromised patients, particularly in those with cirrhosis11).
It has been reported that Aeromonas species are major causative organisms of spontaneous bacterial peritonitis in patients with liver cirrhosis. Early-stage symptoms in peritonitis cases commonly include diarrhea, and concurrent infection with Escherichia coli and Klebsiella can also occur12). During warm seasons (July to September), spontaneous bacterial peritonitis is more frequently caused by Aeromonas species than by other bacteria because of high environmental temperatures, but the incidence rate has recently been decreasing. This can be explained by recent improvements in the water supply and sewage systems11).
In a review of cases of PD-related peritonitis caused by A. hydrophila, coinfection with other bacteria was common. The possible routes of infection may include contact with contaminated well or runoff water and inadequate hand washing. Gut translocation of the bacteria can also occur in the presence of gastroenteritis, colon cancer, or intestinal perforation13). Refractory or relapsing PD-related peritonitis has not been reported. It would be important to determine whether A. hydrophila is a clinically significant organism in PD-related peritonitis through cultures from the environment, including sewage systems, although this has not been performed.
Aeromonas species are susceptible to third-generation cephalosporins, aminoglycosides, aztreonam, fluoroquinolones, and imipenem. However, since there are several reports of resistance, it may be inappropriate to empirically use fluoroquinolone14). When the response to antibiotics is good, Aeromonas species infection generally has a positive clinical outcome, with a low recurrence rate.
In conclusion, we reported a case of automated PD-related peritonitis caused by A. hydrophila, which was cured with intraperitoneal ceftazidime.

 XML Download
XML Download