

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Myelodysplastic syndromes (MDS) are a heterogeneous disease group of clonal hematopoietic stem cell disorders characterized by cytopenia, dysplasia of one or more lineages, ineffective erythropoiesis, and increased leukemia transformation [1]. Azacitidine (AZA) is a hypomethylating agent, approved by the United States and Europe, for treating intermediate-2 and high-risk MDS according to the International Prognostic Scoring System (IPSS) [2]. In multicenter randomized trials, AZA induced a 50-60% overall response, and significantly improved overall survival rate (OS) in high-risk MDS compared to other treatments. Therefore, AZA is currently recognized as the standard of care for patients who are not candidates for allogeneic stem cell transplantation (AlloSCT) [3, 4, 5].
The presence of chromosomal abnormalities (CAs) is a main prognostic factor for the survival of acute myeloid leukemia (AML) and risk of AML evolution in patients with MDS. In recent studies, it has been demonstrated that the complex karyotype (CK) is the most important adverse prognostic survival factor in patients with MDS and AML [2, 6, 7, 8]. In contrast, other investigators have found that the monosomal karyotype (MK), defined by the presence of ≥2 distinct autosomal monosomies or a single autosomal monosomy associated with at least 1 structural abnormality, is associated with poor prognosis in patients with AML or MDS [9, 10, 11]. However, the patient groups in these studies received heterogeneous treatments. A study by Itzykson et al. [12] was performed in patients with MDS treated with AZA; however, the data were limited to only CKs. Therefore, the pure significance of MK or CK as prognostic factors in patients with high-risk MDS treated with AZA is unknown.
We investigated the prognostic value of CAs, such as MK or CK, in patients with IPSS higher-risk MDS who were treated with AZA.
PATIENTS AND METHODS
A total of 243 patients at 6 medical centers (i.e., Pusan National University Hospital, Chonnam National University Hospital, Kyungpook National University Hospital, Chungnam National University Hospital, Gachon University Gil Medical Center, and Gyeong-sang National University Hospital) with IPSS intermediate-2 and higher-risk MDS and who were treated with AZA from September 2006 to February 2013 were enrolled. All patients received at least 4 cycles of AZA after diagnosis. Patients who previously underwent low-dose cytarabine therapy or combination chemotherapy, had an unconfirmed diagnosis of MDS, had an interruption of AZA treatment not owing to an unacceptable response, and received AlloSCT after AZA treatment were excluded. Approval for the retrospective review of records was obtained from the Institutional Review Boards of all participating medical centers.
Cytogenetic study
Cytogenetic abnormalities were classified according to the International System for Human Cytogenetic Nomenclature criteria [13]. Cytogenetic risk was evaluated according to the IPSS classification. According to the criteria of Breems et al. [9], MK was defined as the presence of ≥2 distinct autosomal monosomies or a single autosomal monosomy with at least 1 additional structural abnormality. CK was defined as the presence of ≥3 numerical or structural cytogenetic abnormalities.
Azacitidine treatment
AZA therapy (75 mg/m2/day) was administered subcutaneously over 7 days every 4 weeks for at least 4 cycles. Dose reduction or treatment delay during each cycle was recommended in cases of grade 4 hematologic toxicity. Patients who achieved a response after 4 cycles, according to the 2006 International Working Group (IWG) response criteria, continued treatment until disease progression [14].
Statistical analysis
The overall response rate was measured by the 2006 IWG response criteria. Response duration was measured from the date of bone marrow (BM) biopsy after 4 cycles of AZA in the responders according to the first cell count meeting hematologic improvement (HI) criteria in patients who achieved HI. OS was measured from the start date of AZA therapy to death. Response and survival were estimated according to the Kaplan-Meier method. Comparisons between variables of interest were performed with the log-rank test. Cox regression analysis was performed to determine whether there was a difference in the durable response or survival between the treatment groups. Hazard ratios (HR) and corresponding 95% confidence intervals (CIs) were determined for all survival endpoints. Statistical analyses were conducted with the SPSS software ver. 18.0 (SPSS Inc., Chicago, IL, USA). A P value<0.05 was considered significant.
RESULTS
Patients
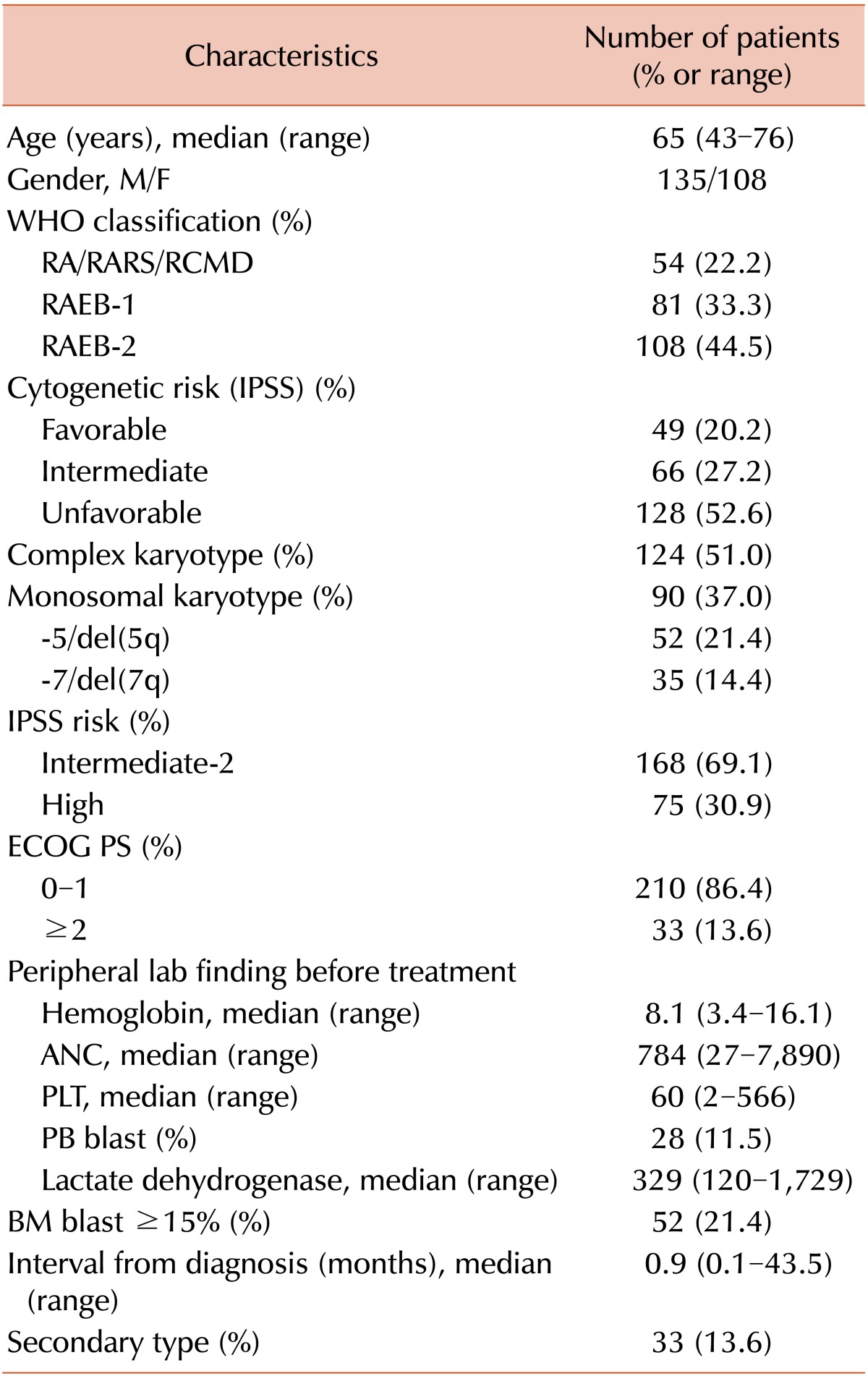
The baseline characteristics of the 243 patients are summarized in Table 1. The median follow-up time for survivors was 24.2 months (range, 4.3-91 months). The median age was 65 years and the male:female ratio was 1.25:1. CK and MK was identified in 124 (51.0%) and 90 (37.0%) patients, respectively. MK with CK was detected in 54 (22.2%) patients and MK without CK was detected in 36 (14.8%) patients. Loss of chromosome 5 (-5) or deletion of the long arm of chromosome 5 (del(5q)) was present in 52 patients (21.4%), whereas loss of chromosome 7 (-7) or deletion of the long arm of chromosome 7 (del(7q)) was present in 35 patients (14.4%). Refractory anemia with excess blast-II type was predominant (108 patients, 44.5%). Cytogenetic risks by IPSS classification were favorable in 49 patients (20.2%), intermediate in 66 patients (27.2%), and unfavorable in 128 patients (52.6%). Thirty-three patients (13.6%) had secondary type of treatment including 29 cases occurring after myeloproliferative neoplasm treated with hydroxyurea and the other 4 cases occurring after chemotherapy for other cancers.
Overall response rate and prognostic factors
All patients underwent a standard schedule of at least 4 cycles of AZA treatment. The median number of treatment cycles was 8 (range, 4-37 cycles). The best response was a complete response (CR) in 45 (18.5%), partial response (PR) in 13 (5.3%), marrow CR (mCR) in 31 (12.8%), and stable disease (SD) with HI in 50 (20.6%) patients (Table 2). The median response duration was 14.1, 15.8, 10.6, and 7.0 months for CR, PR, mCR, and SD with HI, respectively.
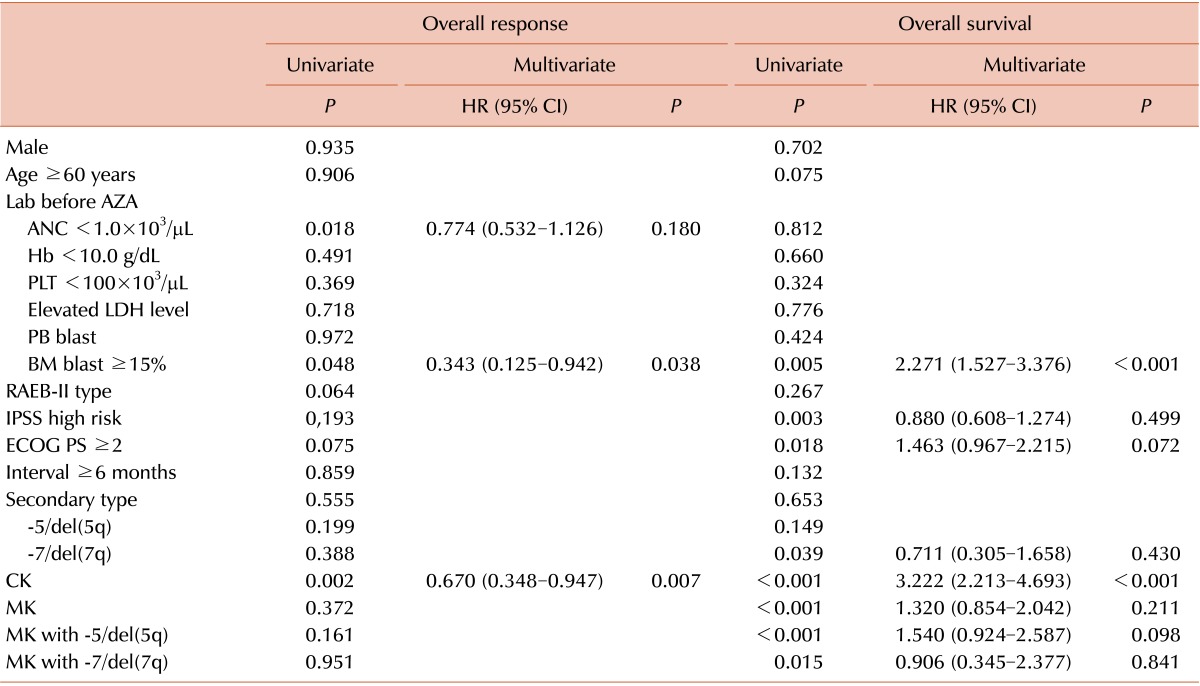
A Cox regression analysis was conducted to determine the prognostic factors that predicted a durable response. In a univariate analysis, the absolute neutrophil count (ANC) <1.0×103/µL (P =0.018), BM blasts >15% (P =0.048), and CK (P =0.002) were associated with a short overall response duration (Table 3). According to the multivariate analysis, BM blasts >15% (HR, 0.343; 95% CI, 0.125-0.942; P =0.038) and CK (HR, 0.670; 95% CI, 0.348-0.947; P =0.007) were independent factors of short response duration (Table 3).
Overall survival and prognostic factors
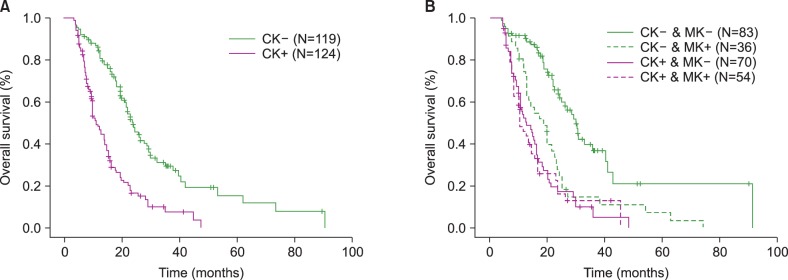
The OS rate was 29.6% in all groups during the follow-up. In the univariate analysis, BM blasts >15% (P =0.005), IPSS high-risk status (P =0.003), Eastern Cooperative Oncology Group (ECOG) performance status >2 (P =0.018), -7/del(7q) (P =0.039), CK (P <0.001), MK (P <0.001), MK with -5/del(5q) (P <0.001), and MK with -7/del(7q) (P =0.015) were associated with low OS (Table 3). In the multivariate analysis, BM blasts >15% (HR, 2.271; 95% CI, 1.527-3.376; P <0.001) and CK (HR, 3.222; 95% CI, 2.213-4.693; P <0.001; Table 3 and Fig. 1A) were independent prognostic factors for low OS.
Impact of monosomal karyotype on survival in patients with/without complex karyotype
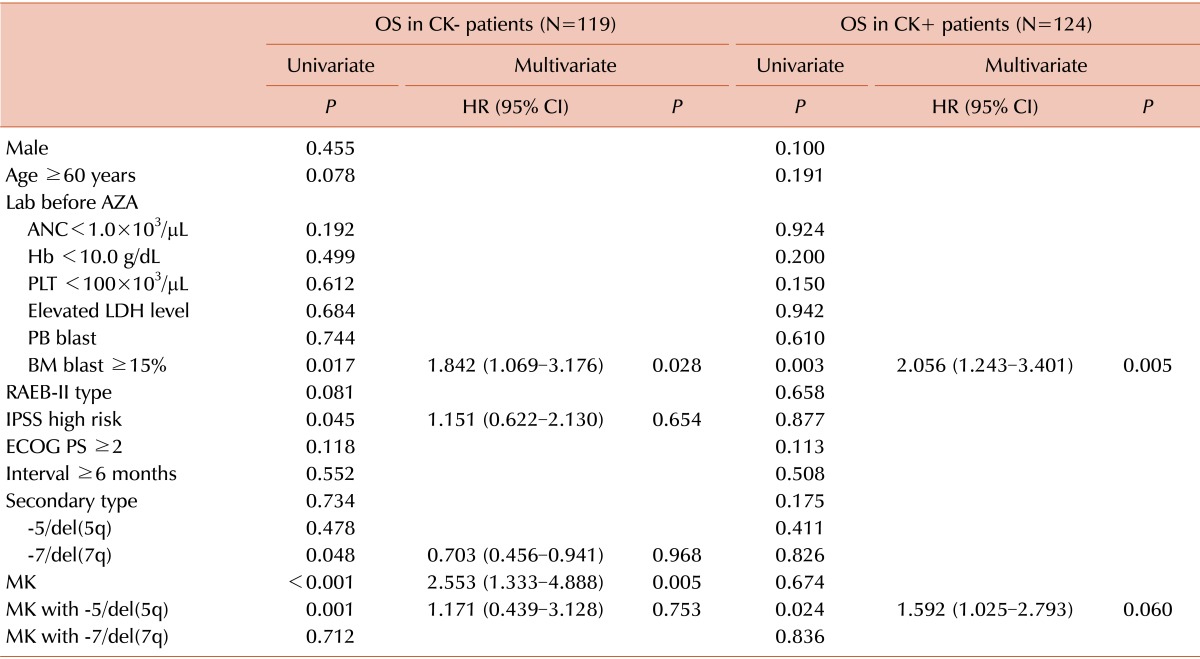
To analyze the impact of MK on OS in patients with or without CK, the entire patient group was separated into 2 subgroups according to the presence of CK (CK- and CK+). In the CK- subgroup, BM blasts >15% (P =0.017), IPSS high-risk (P =0.045), -7/del(7q) (P =0.048), MK (P <0.001), and MK with -5/del(5q) (P =0.001) were associated with low OS. In the multivariate analysis, BM blasts >15% (HR, 1.842; 95% CI, 1.069-3.176; P =0.028) and MK (HR, 2.553; 95% CI, 1.333-4.888; P =0.005) had independent prognostic values (Table 4). However, only BM blasts >15% (HR, 2.056; 95% CI, 1.243-3.401; P =0.005) reflected low OS in the CK+ subgroup in the multivariate analysis. Therefore, a negative status for MK reflected favorable OS only in the CK- group (Fig. 1B).
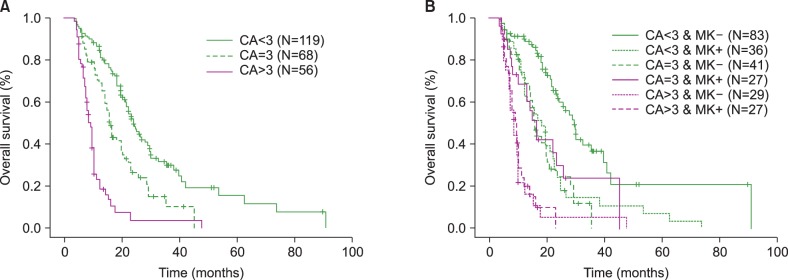
To determine whether the number of CAs would affect OS the patient group was separated into 3 subgroups: CA<3 (N=119), CA=3 (N=68), and CA>3 (N=56). OS was significant according to the number of CAs (median follow-up, 24.2 months; OS, 14.5% in the CA>3 group, 27.9% in the CA=3 group, 37.8% in the CA<3 group; CA>3 vs. CA=3, P =0.001; CA=3 vs. CA<3, P =0.001; Fig. 2A). When the subgroups were divided according to the presence of MK, MK negative status in the CA<3 subgroup was associated with higher OS than the other subgroups (Fig. 2B). However, the MK value was not significant for CA=3 or CA>3.
DISCUSSION
Treatment with AZA lowers the risk of leukemic transformation and improves clinical outcome. However, AZA is considered the standard of treatment for patients with MDS who are not AlloSCT candidates. Therefore, which factors would affect the efficacy and clinical outcome in patients with MDS who are treated with AZA remains unknown.
Although the response duration of AZA was inversely related to IPSS in a previous study, the factor predicting the response was not identified [15]. In a Kantarjian HMstudy about decitabine experience, previous treatment and longer disease duration predicted low CR rates, whereas patients with chromosome 5 or 7 abnormalities, previous treatment, and older age had short survival [16]. CK predicted a poor response in a recent study based on high-risk MDS patients treated with AZA. Furthermore, dependence on red cell transfusions, poor ECOG performance status, intermediate and unfavorable IPSS cytogenetic risk, and the presence of circulating blasts were associated with low survival [17]. Similar results were obtained in the present study, where BM blasts ≥15% and CK were associated with poor response and low survival. CK may be recognized as an adverse prognostic factor in patients with intermediate-2 and high-risk MDS who are treated with AZA. However, AZA treatment may not overcome the IPSS cytogenetic risk stratification in patients with high-risk MDS.
The presence of MK defines an adverse prognostic factor in patients with AML and MDS. Patnaik et al. [10] suggested that MK is associated with poorer OS compared to that of CK. The adverse prognostic impact of MK in patients with MDS or AML has also been shown in other studies [9, 11]. However, this is controversial because it has been determined that MK is a worse predictor of clinical outcome in some studies [12, 18, 19]. Furthermore, these MK studies have been conducted in patients receiving a variety of treatments. Therefore, it is unclear whether MK has prognostic value in patients with MDS who are treated with AZA. Itzykson et al. [12] demonstrated that the MK status among patients with CK who are treated with AZA is not associated with OS. However, their data were limited to those with the IPSS poor risk karyotype. In the present study, a MK negative status in non-CK patients reflected favorable OS. Therefore, the MK status of at least the IPSS intermediate cytogenetic risk group may have a predictive value for the prognosis of patients with MDS who are treated with AZA.
In addition, we found that a high number of CAs affected the clinical outcome of patients treated with AZA.We observed that ≥3 CAs belonged to CK and the CA=3 and CA>3 subgroups had significantly different OSs. Furthermore, the CA >3 subgroup was associated with a worse prognosis in patients with MDS of the IPSS high risk group who were treated with AZA., and the subgroup with >3 CAs was associated with a worse prognosis in patients with MDS of the IPSS high-risk group who were treated with AZA. This result is consistent with the cytogenetic risk stratification (i.e., intermediate, high, and very high risk) of the newly defined and revised IPSS (IPSS-R) [20]. Therefore, cytogenetic risk of the IPSS-R may be more useful compared to IPSS for predicting clinical outcomes in patients treated with AZA. AZA treatment may not overcome the high numbers of CAs related to multiple gene alterations.
The location of CA has been suggested to be prognostic regardless of treatment [18, 21, 22, 23, 24]. However, Itzykson et al. [12] were unable to show that -5/del(5q) or -7/del(7q) in patients treated with AZA has prognostic value. These clinical data were similar to our results. Although the discrepancy among studies is not clearly understood, the presence of MK or number of CAs seems to be more important compared with the location of the CAs in patients with MDS who are treated with AZA.
In conclusion, a high percentage of BM blasts and CK were associated with the worst clinical outcomes. Moreover, MK reflected poor survival in the non-CK patients and >3 CAs was associated with poor survival. Furthermore, well-designed sequential prognostic factor data, including cytogenetics, might allow the identification of risk factors in patients with MDS who are treated with AZA.

 XML Download
XML Download