

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Dear Editor:
Indeterminate dendritic cell tumor (IDCT) is an extremely rare neoplasm derived from indeterminate cells considered to differentiate into Langerhans cells incompletely1.
A 61-year-old man presented with 2-year history of multifocal ulcerative nodules on his back and chest (Fig. 1). We received the patient's consent form about publishing all photographic materials. Each lesion started with a red papule and turned into a necrotic nodule. He stated that he had tried to be treated by surgery in another hospital because the number of the lesions was small at the beginning of the symptom. However, their recurrence in new areas despite repetitive excision allowed him to visit our hospital for a secondary opinion. There was no previous or family history of skin cancers. He denied any subjective symptoms including pruritus and pain.
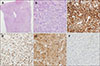
Histopathology revealed heavy infiltrates of round to oval tumor cells, filling up the entire dermis with epidermal sparing (Fig. 2A). Each cell was composed of abundant cytoplasm and various shaped nuclei with fine chromatin (Fig. 2B). Some cells displayed atypical chromatin-rich patterns. Several lymphocytes surrounding the tumor cells but not in the epidermis were found, but eosinophils were obviously absent. The tumor cells represented strong immunoreactivity for CD1a (Fig. 2C), CD68 (Fig. 2D), and S100 proteins (Fig. 2E), but were negative for Langerhans cell markers and follicular dendritic cell markers such as langerin (Fig. 2F) and CD21, respectively. The Ki-67 proliferation index was 70%. Based on the above findings, he was finally diagnosed with IDCT. The patient was transferred to the hemato-oncologic division for further evaluation, and no definite evidence of internal organ involvement was detected. His condition began to improve spontaneously, so he has been on regular follow-up for 3 months without treatment now.
According to the updated version of 2011 on the 2008 World Health Organization classification, IDCT is classified into a group of histiocytic and dendritic cell neoplasms. Due to the rarity of IDCT with only about 80 cases demonstrated before, its etiology has not been well elucidated yet. IDCT can arise de novo, or in conjunction with several diseases including B-cell lymphoma, angioimmunoblastic T-cell lymphoma, and mosquito bites12. IDCT is usually confined to the skin, and occurs in adults without sex predilection3. The diagnosis is very challenging for clinicians and pathologists because of its unfamiliarity, and it is essential to be distinguished from other Langerhans cell lineage tumors such as Langerhans cell histiocytosis (LCH). Tumors cells in IDCT exhibit similar morphology to Langerhans cells with expression of CD1a and S100 proteins1. However, Birbeck granules and langerin are not expressed in IDCT unlike in LCH3. Also, there are lack of apparent epidermotropism and significant eosinophilic infiltration in IDCT, which are characteristic features of LCH3. From this perspective, ultrastructural analysis of Birbeck granules or immunostaining for langerin is regarded to be valuable for accurate diagnosis of IDCT instead of LCH. Chemotherapy, phototherapy or electron beam therapy effectively results in favorable response, but relapse is common after cessation of the treatment 4. Spontaneous regression without recurrence over 17 months to 4 years of follow-up has also been reported in some cases, like our patient25.
Herein, we introduce a case of IDCT, an uncommon neoplasm composed of indeterminate cells resembling Langerhans cells characterized by unique clinicopathological features.

 XML Download
XML Download