

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Q-switched (QS) lasers, which emit high-energy pulses in the nanosecond range at varying wavelengths, have been used with good efficacy for treatment of pigmented lesions. Use of a low-fluence QS neodymium-doped yttrium aluminium garnet (QSNY) laser or ‘laser toning’ has shown efficacy in treating various pigment disorders, including melasma and post-inflammatory hyperpigmentation (PIH) in Asian countries1. However, treatment outcomes are inconsistent, and adverse events such as rebound hyperpigmentation and mottled hypopigmentation have been reported, especially in darker-skinned patients1.
The picosecond laser was introduced in the 1990s, and several studies have shown improved efficacy in clearing tattoo pigments compared with QS lasers2. Moreover, tattoo pigments that are intractable to multiple QS laser treatments have responded to picosecond lasers3. Chesnut et al.4 reported successful treatment of a recalcitrant nevus of Ota with Picosecond 755-nm Alexandrite Lasers. Therefore, we hypothesized that a picosecond laser would show better efficacy with minimal adverse events in the treatment of melasma and PIH that are difficult to treat with conventional QS lasers.
CASE REPORT
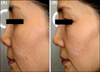
Two patients with melasma and one patient with PIH were treated with a 750-picosecond pulse using a 755-nm Alexandrite Laser (Cyanosure, Westford, MA, USA). All patients were Korean women with skin type IV. All patients had multiple previous low-fluence QSNY laser treatments but were no longer responding to such treatments. Informed consent was obtained for all patients. Two female patients, 53 and 45 years old (patient 1 and 2), had inhomogeneous pigmentation on their cheeks, noses, and temples, consistent with melasma and were treated with a spot size of 6 mm (0.57 J/cm2) for 6 and 14 sessions, respectively, with two-week intervals in between treatments (Fig. 1, 2). One 20-year-old female patient (patient 3) had an ill-defined, 2-cm, brownish patch on her philtrum for more than 3 years that was diagnosed as PIH (Fig. 3). She was treated seven times, two weeks apart, with a 2-mm (5.25 J/cm2) spot size. Laser treatment was well tolerated with minimal downtime. Post-laser erythema was not evident. Neither blistering nor petechia was reported. No patients had developed PIH at 8 weeks after laser treatment. The melasma lesions showed significant improvement at this time (Fig. 1, 2, 3). Patient 1 showed fair improvement and patients 2 and 3 showed good improvement.
An ex vivo skin model from the abdomen of a Korean female was irradiated with a Picosecond 755-nm Alexandrite Laser and a QSNY laser at 532 nm and 1,064 nm. The laser parameters were 1.26 J/cm2 with a 4.5-mm spot size, 1 J/cm2, with a 7-mm spot size, and 3 J/cm2 with a 7-mm spot size, respectively. Immunohistochemical staining using nitro blue tetrazolium was performed 4 hours after the laser treatment to see immediate effect of laser irradiation and detect viable cells. Remaining melanin pigments were quantitatively measured by Fontana-Masson staining 7 days after laser treatment using Image J (National Institutes of Health, Bethesda, MA, USA). Ex vivo experiments results were consistent with clinical outcomes. Four hours after the irradiation, the Picosecond 755-nm Alexandrite Laser led to decreased epidermal keratinocyte necrosis compared with the 532-nm QSNY Laser (Lutronic, Goyang, Korea) (Fig. 4). Quantitative measurements showed that the melanin content was decreased by both the Picosecond 755-nm Alexandrite Laser and the 1,064-nm QSNY Laser (Lutronic) (Fig. 4).
DISCUSSION
The Picosecond 755-nm Alexandrite Laser, which has a pulse duration that is much shorter than the thermal relaxation time of melanosomes, enabled us to selectively and effectively destroy melanosomes while causing minimal damage to surrounding tissues such as vessel hemoglobin and epidermis. Low-fluence 1,064-nm QSNY Laser treatments of melasma or PIH often reach a steady state after multiple treatment sessions. Energy delivery in the picosecond range may achieve more selective photothermolysis of fragmented melanin granules from previous repetitive laser treatments5. With a picosecond laser, lower fluence can be used, which should decrease adverse effects while keeping the peak energy substantially higher than that typically produced by QS lasers. Except its high cost, the picosecond laser has a more favorable effect and safety profile to the QS nanosecond lasers.
In conclusion, the Picosecond 755-nm Alexandrite Laser may be useful for treating melasma and PIH that are intractable to conventional laser toning or residual lesions after QS lasers and shows high efficacy and fewer adverse events in dark Asian skin.



 XML Download
XML Download