

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Androgenetic alopecia (AGA) is the most common type of hair loss1. Both genetic and non-genetic factors are known to play a role in development of AGA2. Many studies have focused on the non-genetic factors of AGA, but few have investigated the association between AGA and exercise. We perform a survey-based study to shed a light on the association among AGA and exercise. This study was approved by the institutional review board of Yonsei University Wonju College of Medicine (YWMR-15-0-071). The subjects visited occupational medical clinic of Wonju Severance Christian Hospital for regular medical check up from October 2012 to March 2015. To minimize the possible influence over AGA other than exercise, the subjects who had any underlying disease were excluded, resulting in 1,182 healthy individuals. Subjects were asked to answer questionnaire about current state of exercise; frequency and intensity of exercise. The intensity of exercise was graded as follows: A) High intensity was defined as more than 20 minutes per day of strenuous physical activity that induces severe shortness of breath; B) Moderate intensity was slightly more strenuous physical activity that induces mild shortness of breath more than 30 minutes per day; C) Low intensity was normal physical activity, such as walking, for at least 30 minutes per day. The frequency of each intensity exercise was defined as the number of exercises carried out per week. Total amount of exercise was defined as sum of frequencies of each intensity. The status of AGA was evaluated through physical examinations by dermatology specialists, and the AGA patients were categorized into several subgroups in accordance with the basic and specific (BASP) classification system3. Differences between normal patients and AGA patients were analyzed using the t-test. A p-value of <0.05 was considered to be statistically significant.
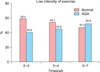
The number of male and female subjects was 600 and 582 respectively (total of 1,182; mean age, 51.38±12.83 years; range, 18~94 years). The number of AGA patients was 534 (45.2%) in total, and 350 (58.3%), 184 (31.6%) within the male and female subgroups respectively. The total amount of exercise was larger in AGA group than that of normal group (p=0.008). When comparing within each exercise intensity group, no significant difference of the amount of exercise between AGA and normal groups was observed in moderate-to-high intensity group. However, within the low-intensity group, the total amount of exercise was larger in AGA group than normal group, with statistical significance (p<0.001, Fig. 1A). We also analyzed the difference between groups with or without AGA family history. Within no AGA family history group, no difference of total amount of exercise was observed between AGA and normal group. However, in low-intensity group, the frequency of exercise was higher in AGA group than in normal group (p=0.018, Fig. 1B). On the other hand, total amount of exercise was larger in the positive AGA family history group (p<0.001). According to the intensity of exercise, higher frequency of exercise was observed within moderate and low-intensity groups (p=0.014, p<0.001, respectively). Whereas no significant difference was observed within high-intensity group (Fig. 1C).
The proportion of alopecia was compared according to exercise intensity and frequency. The frequency of exercise was assorted into 3 groups (0~2, 3~4, 5~7 times a week). No association among alopecia and exercise frequency was observed in moderate-to-high intensity group. However, a tendency of increasing proportion of alopecia patients was observed in the low-intensity exercise group as exercise frequency increased (Fig. 2). No difference was observed alopecia types (accrording to the BASP classification system3) and exercise. In addition, the severity of alopecia was not associated with exercise.
According to the results of this study, alopecia patients exercise more than the normal population, especially low-intensity exercise. Similar tendency was observed irrespective of the family history of AGA. Also the proportion of AGA patients showed an increasing trend as the frequency of exercise of low intensity increased. During the exercise, the testosterone level could be increased transiently4. However, as the subjects in this study were required to answer their lifelong exercise habit, long-ranged changes in hormone level would be more importance over the transient ones. According to a study, no differences in serum cortisol, total testosterone and free testosterone level were observed between lifelong exercise and no exercise group5. Accordingly, we hypothesized that factors other than changes of hormone level would take an important part in the occurrence of alopecia. If it could be assumed that exercise could induce alopecia, we conjectured that oxidative stress which is generated during exercise plays an important role in the process. Oxidative stress increases the entry of dihydrotestosterone into the dermal papillary cells, and reactive oxygen species (ROS), associated with oxidative stress, increase 5α-reductase concentration and activity67. However, as the amount of ROS generated during exercise is larger in more intense exercise8, this explanation for the association between exercise and AGA is limited. However, according to a study of Parker et al.9, regular moderate-to-high intensity exercise can induce a protective effect against oxidative stress, by elevating endogenous antioxidant defense mechanisms. This protective effect is a possible explanation for the significant association observed only in the low-intensity group.
This is the first large-scale study to analyze the association between exercise and alopecia. According to this study, there is an apparent association between exercise and alopecia. However, as of the result of an observational study, it cannot be confirmed that alopecia or exercise preceded the other. Therefore, the results of our study do not demonstrate causality between exercise and alopecia. We suggest ROS hypothesis as one of possible explanations between low-intensity exercise and the occurrence alopecia. Further study which places more emphasis on comparing the frequency of occurrence of alopecia in regular and non-regular exercise group is necessary to support ROS hypothesis. Surely, the occurrence of alopecia is influence by numerous genetic and environmental factors, and we agree that ROS theory cannot be a ‘one and only’ answer. We are suggesting ROS hypothesis as one of possible explanations influencing occurrence of alopecia, and further study is necessary to confirm the associated pathophysiology.

 XML Download
XML Download