

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Focal dermal hypoplasia, also known as Goltz syndrome, is a disorder associated with mutations in the PORCN gene and has X-linked recessive inheritance. Affecting organs originating from the mesoderm and ectoderm, focal dermal hypoplasia is characterized by skin changes and abnormalities in the ocular, oral, neuropsychiatric, and musculoskeletal systems. The skin lesions resemble atrophic patches arranged in a linear fashion following Blaschko's line. The lesions change to brown- or yellow-colored nodules in response to fat cell deposits.
Focal dermal hypoplasia is a relatively rare disease; there are only seven previous reports from the Republic of Korea. However, the unilateral or almost unilateral form, wherein the clinical manifestations are mostly limited to one side of the body, is extremely rare. To our knowledge, there have been only seven reports of this unique form of focal dermal hypoplasia in the world and there are no previous reports from Korea. Herein, we report on a 19-year-old female who had almost unilateral focal dermal hypoplasia on the right side of the body with concomitant aplasia cutis congenita and syndactyly.
CASE REPORT
The patient was a 19-year-old woman who was born with a scalp defect. The defect healed after conservative wound management early in her life. She had no specific medical history and no signs of neuropsychiatric problems. Neither her parents nor brothers had dermatologic or systemic problems.
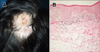
She first visited our clinic for evaluation of her scalp lesion 10 years ago, when she was nine years old. The scalp lesion had been replaced by fibrotic tissue and appeared to be an atrophic alopecic patch (Fig. 1A). Examination of skin biopsy specimens from the scalp showed an irregularly thickened epidermis, atrophic dermis with upward extension of the subcutaneous tissue, and mild fibrotic changes and loss of periadnexal structures (Fig. 1B). A diagnosis of aplasia cutis congenita was made based on clinical and histologic features.
During the 10 years after her last visit, atrophic and nodular skin changes on the right side of the trunk and limbs began to appear and become progressively more prominent, while the syndactyly of the right fourth and fifth toes, which had not been identified previously, was negatively influencing her quality of life. Thus, the patient returned to our clinic and a complete physical examination of the body was performed. We identified multiple, variously sized, and well-demarcated atrophic patches that were mostly confined to the right trunk and leg (Fig. 2A, B). Some lesions appeared as brown or yellow protruding masses, and were accompanied by deposited and herniated fat tissue. The atrophic patches and protruding masses were arranged in a linear fashion following Blaschko's line. We observed only a few atrophic patches on the patient's left leg. We also noted the syndactyly of the right fourth and fifth toes (Fig. 2C).
A skin biopsy from the right calf revealed prominent dermal atrophy and extension of subcutaneous fat toward the upper dermis (Fig. 3). Focal dermal hypoplasia, also known as Goltz syndrome, was diagnosed on the basis of clinical and histologic findings. Because most of the skin lesions were confined to the right side of the body, the focal dermal hypoplasia in this case was identified as the almost unilateral form.
Because the patient complained of discomfort from syndactyly of her right fourth and fifth toes, we referred her to the Department of Plastic and Reconstructive Surgery to surgically manage this condition.
DISCUSSION
Focal dermal hypoplasia, discovered by Goltz in 1962, is a genodermatosis that involves abnormalities in the mesodermal and ectodermal organs. Clinical manifestations vary from minimal skin changes to global defects in multiple organ systems that can lead to death12. Patients are almost always female because focal dermal hypoplasia is an X-linked recessive condition, originating from a mutation of the PORCN gene located in Xp11.23. The PORCN gene involves encoding of O-acetyltransferase through an association with the Wnt signaling pathway; consequently it plays a critical role in the proliferation and development of bone tissue3456.
Skin lesions seen in focal dermal hypoplasia cases appear as linear and atrophic patches that occur secondarily to dermal atrophy and brown or yellow protruding masses that emerge due to fat cell deposition and herniation. Abnormalities in the musculoskeletal system, such as syndactyly, oligodactyly, adactyly, scoliosis, spina bifida, and clavicular hypoplasia, are the most common extracutaneous manifestations. Dental problems, such as enamel hypoplasia or oligodontia, are seen in over half of focal dermal hypoplasia patients and these can be accompanied by ocular problems, such as strabismus and micropia, as well as abnormalities of the brain and spinal cord, or other neuropsychiatric problems7.
Because the patient initially presented with congenital scalp defects, she was diagnosed with aplasia cutis congenita. However, aplasia cutis congenita is often associated with malformation syndrome, including focal dermal hypoplasia, and is classified in group IX according to Frieden's classification8.
Focal dermal hypoplasia has been reported in over 250 cases and in seven in the Republic of Korea. Globally, there have been only eight reported cases of unilateral or almost unilateral focal dermal hypoplasia.
The majority of patients were female and only one was male9 among eight patients. Abnormalities in the internal organs or neuropsychiatric problems are relatively common symptoms of focal dermal hypoplasia. However, involvement of internal organs among unilateral and almost unilateral cases occurred only in male patient and none of the patients had mental retardation or other psychiatric problems9101112131415. Our patient did not show any signs of systemic or neurologic involvement (Table 1). When considered with previous findings, the evidence suggests that unilateral or almost unilateral focal dermal hypoplasia is less likely than the classical form to manifest in the internal organs or the neuropsychiatric system. However, due to the small number of available cases, further studies and case collections are needed to verify this conclusion.
Gene sequencing was performed for a case of almost unilateral focal dermal hypoplasia reported by Maalouf et al.14 and a heterozygous mutation was found in exon 10 (c.854855insACCTGAC[p.T285fsX316]) that results in premature signal halting. X-chromosome inactivation analysis was also performed and DNA from apparently healthy skin of the right arm (normal side), healthy skin of the left arm (involved side), and lesional skin from the left arm had a pattern of random inactivation ratio of 44:50, 72:25, and 87:13, respectively. A different mutation of exon 14 (c.1179_1193del) was found in the almost unilateral case reported by Asano et al.15.
It is thought that pathogenesis is different between the unilateral or almost unilateral form and the classical form of focal dermal hypoplasia. However, there are many heterogeneous mutations associated with classical focal dermal hypoplasia, so it is difficult to describe the respective pathogenic pathways of the two different forms; more studies, including genetic analyses, are needed.
Regular follow up is needed for early detection and treatment of anomalies from focal dermal hypoplasia. Some reports suggest that treatment with a 588-nm flashlamp-pumped pulse-dye laser is effective for erythematous and telangiectatic skin lesions16. Surgical management targeted toward individual abnormalities may also be needed to improve patients' quality of life.



 XML Download
XML Download