

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Milia are small, epithelium-lined keratinous cysts in the dermis thought to result from plugging of pilosebaceous or eccrine sweat ducts. Milia present as 1~2 mm, white, domed papules, most commonly on the face. They may appear spontaneously (primary milia) or after clearing of inflammatory skin diseases and trauma (secondary milia)1. Multiple eruptive milia represent an unusual condition in which numerous lesions develop suddenly on the face and trunk. We describe a case of multiple eruptive milia spontaneously occurred in unusual sites in a 19-year-old girl.
CASE REPORT
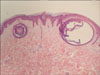
A 19-year-old girl presented with asymptomatic, white papules on the abdomen and in both axillae that began to develop 5 years prior to her presentation. The patient was otherwise in good health, and there was no history of trauma or excessive exposure to sunlight. No similar eruptions were noted in family members. Cutaneous examination revealed multiple, white, firm, discrete, 1~2 mm papules on the abdomen and in both axillae (Fig. 1). Histologic examination of the lesions revealed two subepidermal keratin-filled cysts lined with stratified epithelium(Fig. 2). No treatment was desired or administered.
DISCUSSION
Milia can be classified as primary or secondary. Primary milia develop spontaneously and are common on the faces of newborns. Primary milia may also be present on the trunk and extremities. In children and adults, primary milia are found mainly on the eyelids and cheeks. Secondary milia may occur anywhere following trauma, for example burns, subepidermal blistering diseases, dermabrasion, radiotherapy, or following topical therapy with glucocorticoids or 5-fluorouracil1. Secondary milia may also be associated with certain genodermatoses. Other patterns of milia include milia en plaque and multiple eruptive milia. Milia en plaque is characterized by multiple, minute, white papules within an erythematous plaque, commonly located on the ears2.
The first report of multiple eruptive milia was published by Miescher3 in 1957. Miescher3 described a case of multiple eruptive milia associated with multiple trichoepitheliomas on the face, thought to be an example of the multiple trichoepithelial syndrome. Langley et al.4 classified multiple eruptive milia into three categories: 1) spontaneous without a known cause or association (i.e., idiopathic); 2) a familial pattern with autosomal dominant transmission, and, 3) a component of a genodermatosis. Only six cases of idiopathic multiple eruptive milia have been reported in the English literature (Table 1)4-9, and two cases have been reported in the Korean dermatologic literature10,11. Reported sites of occurrence include the face, scalp, neck, upper trunk, shoulders, and arms. This is the first reported case of idiopathic multiple eruptive milia on the abdomen and axillae. Formerly, the localization of multiple eruptive milia to sun-exposed areas, such as the head, neck, and chest, led some authors to suggest sunlight as a precipitating factor4. As our patient developed milia in non-sun-exposed skin, however, we suggest that stimuli other than sunlight play a role in the pathogenesis of multiple eruptive milia. The causative factor for multiple eruptive milia remains unclear. However, external stimuli such as friction or rubbing may cause invaginations of epidermal cells and result in multiple eruptive milia.
Multiple eruptive milia have also been described in families with autosomal dominant transmission4. Published cases include a father and son presented with eruptive milia on the face, neck, shoulders, upper back, and axillae who were otherwise healthy12, and a mother and son with lesions on the face and upper trunk13. In the latter, the son also had striate leukonychia. Multiple eruptive milia have also been reported in association with genodermatoses, such as the basaloid follicular harmatoma syndrome, Rombo syndrome, Bazex syndrome, orofacodigital syndrome I, and Gardners syndrome1.
Differential diagnoses of multiple eruptive milia include miliaria crystallina, eruptive syringoma, eruptive vellus hair cyst, and verruca plana. Generalized idiopathic calcinosis cutis mimicking multiple eruptive milia has also been reported, and requires differentiation14. Commonly administered treatment modalities for milia include excision, followed by extrusion of the keratin core, carbon dioxide laser, curettage, mild electrocautery, and electrodessication9. Successful treatment has also been reported with topical tretinoin and ER: YAG laser1.
In summary, we report our experience of a patient with a 5-year history of multiple eruptive milia on her abdomen and in her axillae with no definite causative factor, which represents a rare case of idiopathic multiple eruptive milia that occurred in unusual sites.


 XML Download
XML Download