

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Porokeratosis is a group of disorders of keratinization that is characterized histologically by a parakeratotic column in the center of a keratin-filled invagination, called a cornoid lamella. Clinically, the basic lesion is sharply demarcated and hyperkeratotic with central atrophy. The pathogenetic mechanism of porokeratosis is still unknown, but porokeratosis is known as genetically heterogeneous disorder associated with UV light, trauma, infection, and immunosuppression1. Besides the classical porokeratosis of Mibelli, there are also five clinical variants: porokeratosis palmaris et plantaris disseminata (PPPD), linear porokeratosis, punctate porokeratosis, disseminated superficial porokeratosis (DSP), and disseminated superficial actinic porokeratosis (DSAP), all of which may be inherited by autosomal dominant mode.
DSP is a rare variant and is characterized by asymptomatic, small, annular papules that involve the trunk, genitalia, palms, and soles. Lesions range from 2 to 5 mm in size and an excess of 100 lesions may be present, but do not spare sun-protected area as in DSAP. The histological typical features of porokeratosis, cornoid lamella and vacuolated keratinocytes, are less pronounced in DSP than in classical porokeratosis of Mibelli. In many cases of DSP, the presence of immunosuppression has been an eliciting factor.
We report an unusual case of disseminated superficial porokeratosis in a patient with gastric cancer.
CASE REPORT
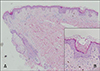
In July 2005, a 65-year-old man visited our department for evaluation of numerous round brownish macules and patches with slightly elevated rims on the trunk, face, and limbs that had developed about 1 year before his examination (Fig. 1). There was no associated pruritus or pain. A clinical diagnosis of disseminated superficial poro-keratosis (DSP), but not disseminated superficial actinic porokeratosis (DSAP), was made because the lesions were located not only in sun-exposed areas but also in sun-protected areas including the trunk. A skin biopsy specimen taken from the elevated rim of a lesion on the patient's abdomen revealed cornoid lamellae and some necrotic keratinocytes, which were consistent with porokeratosis (Fig. 2). Laboratory tests including liver function tests and kidney function tests showed no remarkable findings.
In June 2004, he had presented to the Department of Internal Medicine with abdominal discomfort. A diagnostic gastrofiberscope showed an elevated lesion on the stomach wall, and additional diagnostic evaluations including endoscopic biopsy and computed tomography revealed his lesion as early gastric cancer, poorly differentiated type. Subsequently he underwent surgical treatment, a subtotal gastrectomy, and no further treatment was needed.
At about the same time that early gastric cancer was diagnosed, disseminated skin lesions developed. He said he had had similar skin lesions for some time prior to his visit to our department. However, the previous lesions were scattered just on the trunk, not disseminated, and the rims of the lesions were not accentuated. Thus we determined that the DSP developed almost concurrently with diagnosis of gastric cancer.
He revisited our department in June 2007 with slightly improved lesions. During the 2 years following the gastrectomy, he had received no further treatment for the gastric cancer, and the skin lesions did not increase in size or number. They responded modestly to topical steroids.
DISCUSSION
hereditary factors and additional exogenous factors. An autosomal dominant mode of inheritance with reduced penetrance has been established for porokeratosis of Mibelli, PPPD, and DSP. In genetically predisposed skin, additional factors are assumed to trigger the clinical manifestations. Irradiation with ultraviolet light, organ transplantation23, bone marrow transplantation4, chronic hepatic failure5, renal failure6 and HIV infection7 are thought to be triggering factors.
In our patient, there was no family history of porokeratosis and no remarkable medical history except early gastric cancer. Furthermore, the skin lesions suddenly spread all over his body simultaneously with the diagnosis of gastric cancer. Therefore the DSP lesions seem to have occurred as a paraneoplastic phenomenon associated with gastric adenocarcinoma.
Several cases with rapid extension of DSP have been reported in patients with chemotherapy and bone marrow transplantation, which are associated with immunosuppression1. Moreover, DSP are often recognized after hematopoietic malignancies but there are few cases of development of DSP in patients with cancer of visceral organs. Lee et al8 reported DSP in a patient with cholangiocarcinoma and Takata et al9 reported hereditary non-polyposis colorectal cancer associated with DSP.
Gastric cancer is very common in Korea, being the leading cancer type accounting for 20.8% of all malignant neoplasms and the second leading cause of cancer deaths10. Several risk factors are involved in the development of gastric cancer including diet, gastritis, intestinal metaplasia, and Helicobacter pylori infection. In addition, inactivation of the p53 gene may play an important role in gastric tumorigenesis by loss of suppression of cancer cells11. A negative regulator of p53 function, mdm2, is also associated with molecular pathogenesis of gastric cancer12. In porokeratosis, too, overexpression of p53, decreased mdm2, and dysregulated cell cycle are pathogenically implicated13.
Shumack et al14 reported that hyperproliferative state of keratinocytes in porokeratosis is influenced by inflammatory mononuclear infiltrate, composed of helper T cells and suppressor T cells, located beneath the epidermis. Soluble factors released by activated T cells may provide a mitotic stimulus for overlying keratinocytes. Gastric cancer cells have been reported to secrete several cytokines including transforming growth factor (TGF)-α1516, interleukin (IL)-6 17, and IL-8 18. Thus, we speculate that these cytokines secreted by gastric cancer cells may play a role in the proliferation of keratinocytes, leading to increase in size and number of DSP lesions.
This case demonstrates the importance of thorough systemic work-up in patients with sudden appearance of DSP.

 XML Download
XML Download