

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Diabetes mellitus (DM) is known as the most prevalent metabolic disorder caused by the inability of the pancreas to produce insulin sufficiently or the body's lack of ability to use insulin effectively. There are various factors that cause diabetes, such as diet, lifestyle, and genetics [123456]. Despite healthcare advances, the prevalence of diabetes is still growing, and currently, more than 200 million people worldwide are affected by DM [789]. The number of patients with diabetes, estimated by the World Health Organization (WHO) in 2004, was expected to rise from 171 million in 2000 to 366 million by 2030 [101112]; however, the recent estimation by the International Diabetes Federation (IDF) indicates that the number of diabetic patients will increase to 552 million by 2030 [51314]. DM can cause many complications, such as damage to the heart, blood vessels, eyes, kidneys, and nerves [515]. As a serious health concern, DM has been declared a global epidemic by the WHO due to its rapidly increasing incidence. Nowadays, many multidisciplinary studies are being done to support the prevention and treatment of DM, and it has become a worldwide research priority [516]. Thus, the surveillance, prevention, and control of diabetes and its complications using two or more disciplines are becoming increasingly important [3517] As each discipline has its own potential and added value, the combination of them might be a solution for DM [18].
Artificial intelligence (AI) has been applied in various medical fields for many purposes. Actually, AI is defined as “a field of science and engineering concerned with the computational understanding of what is commonly called intelligent behavior with the creation of artifacts that exhibit such behavior” [1920212223]. AI algorithms have the potential to deliver better care especially in combination with recent technologies [24]. Because modern medicine has faced challenges regarding a large amount of data acquisition, analysis, and the application of the obtained knowledge to solving complex clinical problems, it is necessary to use AI capabilities for these purposes [192125]. AI is composed of various intelligent algorithms and techniques, such as machine learning (ML), natural language processing (NLP), robotics, fuzzy logic (FL), expert systems (ES), knowledge base (KB), and the mix of two or more methods (multimethods) [2123]. ML methods are common with the ability of conducting these two tasks including either prediction (when the outcome variable is a value) or classification (when the outcome variable is a class) [26]. These tasks may also be applied in DM care for disease probability prediction, screening, diagnosis, treatment guidance, and complication management [19212728]. Several ML methods as a subcategory of AI have been applied to fulfill these clinical purposes using their own specific capabilities [2930]. In detail, they include many techniques, such as artificial neural networks (ANN), support vector machine (SVM), decision tree (DT), and naive Bayes (NB), for prediction or classification of clinical outcomes. In routine medical practice, AI in medicine has been linked to the development of programs to help physicians in formulating diagnoses, making therapeutic decisions, and predicting the critical status, such as an emergency or worsening of a patient's condition, in their everyday duties [17222429]. Considering the importance of type 2 diabetes mellitus (T2DM) care as well as assuming that AI applications for diabetes care are effective tools, also due to a lack of studies to investigate the application of AI for T2DM care, this study reviewed AI algorithms and techniques for T2DM care with a specific focus on machine learning methods.
II. Methods
1. Research Question
This study aimed to identify AI applications in T2DM care. We reviewed papers that have reported the methods and techniques of AI in T2DM care. The study population comprised people with T2DM, the intervention was using AI for health-related applications in the area of T2DM; the comparison was excluded; outcomes were the identification of various methods and techniques using AI in T2DM care.
1) Search strategy
This study was a review that was conducted in 2018. Searches were done in scientific databases, including PubMed, Web of Science, and Embase, based on the combination of related keywords based on mesh terms (Table 1). All steps of searches were done based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. The searches were done by two researchers independently to prevent possible bias. The search results referred to a third person who reviewed contradictions, and made decisions in cases where there were disagreements.
The searches were limited to papers published in the English language and a 5-year period of time (2012–2017).
2) Inclusion and exclusion criteria
The inclusion criteria were original articles, clinical trials, and meta-analysis reports. Also, those works that had model performance evaluation, such as accuracy, sensitivity, specificity, and area under the curve (AUC) were included. Exclusion criteria were non-English articles, unavailable full text, other study types except clinical trial, and meta-analysis. Other article types included review articles, letters to editors, short communications, etc. Also conference articles were excluded. Non-human-study papers and papers without model performance evaluation criteria were removed.
3) Selection process
The process of article selection was based on PRISMA (Figure 1). Finally, 31 papers were selected. All steps in the selection and evaluation of the quality of the papers were done by two researchers. Cases of disagreement were referred to a third person to make the final decision. The data extraction form had eight categories, including the author's name, publication year, AI methods applied, algorithms used, health applications for T2DM, clinical variables, optimal algorithms, and the best performance of the model based on the related indexes. After data extraction, we summarized and reported the findings in tables and figures according to the objectives of the study.
III. Results
According to the study search terms, 31 papers were reviewed in details. Table 2 showed the breakdown of articles categories. Most of the papers (n = 9) were published in 2016. Table 2 presents information about the selected studies.
In this study a variety of variables were considered, as shown in Table 2. They comprised the following: (1) AI methods (ML, KB, ANN, FL, ES, NLP, and robotic); (2) in case that the applied AI method was ML, we analyzed the algorithms of ML (ANN, SVM, NB, etc.); (3) we also studied the AI applications of health aspects for T2DM (risk factor analysis, screening and diagnosis, treatment, nephropathy, neuropathy, diabetic foot, etc.); (4) clinical variables were clinical features which were applied to be analyzed by using AI methods; and (5) the best performance values of mathematics models were listed and compared. For this purpose, we only studied those papers with reported performance values as inclusion criteria.
As shown in Figure 2, 71% of papers applied ML, 23% used multiple methods, and just 6% of them used the KB method. Results show other methods, such as FL, ES, NLP and robotic, have not been applied to T2DM separately.
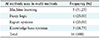
Table 3 shows the frequency of AI methods used when multiple methods were used. In 16 articles, two or more AI methods were used for T2DM concurrently. ML (n = 5) was the most frequently used method together with other AI techniques.
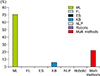
Figure 3 shows the frequency of algorithms applied specifically in ML. In 51 cases, ML algorithms were used for T2DM care. As seen in Figure 3, SVM was the most frequently used algorithm. NB was the second most commonly used algorithm. Moreover, the results show that logistic regression, which is one of the most famous statistical algorithms was applied in 13 cases in the reviewed research.
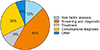
Figure 4 shows the frequency of AI applications to health aspects of T2DM. The results showed that the most common medical application of AI for T2DM care was in screening and diagnosis, with a 45% frequency. Then, complication diagnosis was the next most frequent application of AI (26%).
IV. Discussion
According to the results, the main AI applications are related to ML use for knowledge production and model development, which has been widely used in many healthcare applications [9]. It is a key technology to transform biomedical datasets into actionable knowledge that is useful for the advancement of clinical practice and healthcare through rules developed by medical experts, statistical methods, and ML algorithms with the ability of self-improvement [93061]. Actually, ML methods often achieve high accuracy due to looser assumptions regarding data distribution in comparison to other methods [810111730]. The results of this study indicate that main clinical variables in running and designing ML models and systems for type 2 diabetes care, were body mass index (BMI), fasting blood sugar (FBS), blood pressure (systolic and diastolic), HbA1c, triglycerides (TG), low-density lipoprotein (LDL), high-density lipoprotein (HDL), family history, and demographic variables (Table 2). This study supports the evidence from previous reports that have identified some important clinical variables that are used in data mining methods in diabetes research [29].
According to the results of this study, models based on ML algorithms in T2DM care have been mainly focused on pre-diabetes screening and diagnostic outcomes, risk factor analysis, treatment, and complication categorization. That is, ML algorithms have been mainly used to classify diabetic prone cases for pre-diabetes, diabetes, and advanced diabetes based on the patients' HbA1c level. They are used to analyze T2DM risk factors in various populations to determine which categories of patients may require more attention to prevent (1) disease occurrence, (2) progress to worse stages, and (3) advancing to complications [2951]. This study revealed that there has been limited research on estimating the probability of these outcomes rather than classifying patients based on their disease outcomes in the given three categories. According to previous classification experiments, SVM, which has been widely used for diabetic data analysis has outperformed other algorithms. This may be attributed to its capability to apply hyperlinks to separate classes in a three-dimensional space [6162]. Also, NB, which has been used in several cases for the purpose of determining diabetes-related outcomes is usually applied for prediction task only for small datasets [29]. Using this algorithm, the probability of specific outcome occurrence, such as pre-diabetes occurrence probability, can be calculated; while by using the algorithm of NB the probability of specific outcome occurrence such as pre-diabetes occurrence can be calculated, there is no report of conducting this work in practice. Generally, ANN, and DT in the frame of C5, CART, and RF have been applied for both classification and prediction purposes [6364]; however, there has been no report of applying these algorithms for diabetes-related outcome prediction using big data, even with a satisfactory and generalization level.
The performance of AI techniques and its models applied to T2DM care are shown in the eighth and ninth columns of Table 2. Regarding the best performance of ML techniques, it is obvious that there are no particular best techniques for every condition. For example, decision trees that classify cases by sorting them based on feature values show varying performance in different studies. It has been reported that there is a relationship between the performance of applied techniques and the following subjects, including the type of issues analyzed, the type of input data (discrete or continuous), and finally, the emerging overlapping in outcome classes [656667].
In the area of AI application for T2DM care, there have been some scattered observational studies which need more trials to be applied in routine care. For example, a study presented a patient-level sequential modeling approach to implementing personalized prescription. In this approach, previous records of a patient were applied to the prediction of future prescriptions to improve accuracy. The effectiveness of this method was tested by implementing prediction models based on recurrent neural networks (RNN) [68]. Another study performed a literature review of efforts to use artificial intelligence techniques for diabetes management. The results demonstrate that AI methods are not only suitable for use in clinical practice but also self-management of diabetes. Also, these methods have the potential for improving patients' quality of life [24]. The present study focused on ML techniques to predict T2DM outcomes. The frequencies of various types of applications, as well as health aspects of T2DM care, were studied. Other AI methods may provide additional powerful tools to support diabetes care.
Furthermore, an experiment used the Q-learning algorithm in the area of reinforcement learning of AI to develop personalized treatment plans based on glucose level to provide different basal dose levels automatically for the treatment of each diabetes patient. This approach is a model free of reinforcement learning technique, which is used to determine the optimal treatment policy from a patient's treatment history and related laboratory results. The results reveal that this approach is an effective tool for personalized diabetes management [69].
As seen in Table 2, there have been several reports of multiple-method applications in T2DM care. Most of the ML algorithms have been used with FL, KB, and ES to create multiple-method-based systems for users in the area of diabetes control, including patients, physicians/nurses, managers, and policymakers. In the frame of these systems, ML applications for T2DM data analysis are used for knowledge production to enrich the system's knowledge base incrementally. They use diabetes patients' real data collected in a data repository over time to create a rich knowledge base. The knowledge base might also include experts' knowledge. The fuzzy method can either use real data or experts' knowledge to enrich the knowledge base [70].
Similarly, robotics technologies learn from humans and from the environment [71]. Despite many applications of ML in the framework of an indirect ES or direct ES, according to our inclusion criteria, there have been no reports of studies using robotics and NLP technology to support T2DM care that have evaluated model performance at the same time.
There have been reports on other areas of DM research using robotics, such as using a robot for pancreas transplantation, pancreatectomy surgery, and monitoring and training to improve the care of elderly with dementia [727374]. Also, the management of type 1 diabetes in children is improved by robots. Robots can keep track of individuals' performance and can offer tailored lessons to enhance learning [75].
One of the most interesting findings of this study was that AI has often shown success in the prediction of related issues in T2DM. For example, in treatment, a study predicted DPP-IV inhibitors with ML approaches with 87.2% accuracy [31]. In screening and diagnosis, another investigation predicted hypoglycemia using ML models with 97% accuracy [40]. In the diagnosis of complications (nephropathy), a study predicted microalbuminuria using multiple AI methods (ML, FL, ES) with 92% accuracy [45]. In risk factor analysis, another study predicted the risk of type 2 diabetes, hypertension, and comorbidity using ML models with 85% accuracy [58].
The results of this study may support researchers and developers of AI-based systems and models in the care of patients with T2DM in choosing methods, models, algorithms, and efficient and optimal systems. It is suggested that ML, specifically SVM and NB, algorithms are considered by designers and developers of patterns and systems. The present study also identified the most important clinical variables used in the design and development of artificial intelligence systems and models for the care of patients with T2DM. This can provide insights for choosing key variables in T2DM, and in data analysis and system development using AI-based methods.
One of the limitations of this study was the number of databases that were reviewed. In this work, PubMed, Embase, and Web of Science were reviewed. In fact, the focus of this review was clinical databases; therefore, more technical databases, such as IEEE and Scopus should be considered for further reviews. Future investigation should focus on the effect of AI on clinical outcomes and its impact.




 XML Download
XML Download