

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
X-rays have been widely used in medical examinations since their discovery by Wilhelm Conrad Roentgen in 1895 [1]. Various other medical imaging methods, such as computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) have been developed and have replaced the use of X-ray imaging for some functions. However, X-ray remains the most common medical imaging tool. Especially, the chest X-ray, which reveals the lungs, heart, and bones, is one of the most common chest imaging protocols. The advent and advances in computer technology have spurred interest in the exchange of medical record between medical centers and more effective management of medical records using computers and communication systems. Based on the interests, electronic medical record (EMR) systems and picture archiving and communication systems (PACSs) have been proposed [2,3].
Despite the allure of computation data collection, exchange, and management, X-ray information is still collected as narrative reports in free-text form [4,5]. Electronic standardization and exchange of X-ray clinical information effectively requires the interlocking of the standardized chest X-ray observation system with PACS and/or EMR. Natural language processing [4-6] and standardized methods such as clinical model-based [7-10], have been proposed. However it is often difficult to use and/or need improvement in various cases [7].
Therefore, to simplify the exchange of clinical X-ray diagnosis information according to patients and to standardize the diagnosis report form, we herein propose a simple X-ray observation entry system that can be interlocked with EMR and PACS. The proposed system consists of patient lists, an observation result entry component composed of radio buttons and a chest X-ray image view module. Using this chest X-ray observation entry system, it is possible to extract the observation results in an Excel format, which enables both construction of a data mart and further research using computer-aided decision tools.
The rest of this paper is organized as follows: In section 2, we show the composition of the proposed entry system. In section 3, we show the implemented entry system, and, finally, In section 4 concludes this paper.
II. Case Description
1. Conventional Methods
The conventional EMR system is based on free-text. Therefore, it is impossible to reuse and/or exchange the medical information. To overcome this drawback, structured entry support systems have been proposed and studied. The key purpose of these methods is to construct structured data set for effective medical information exchange and practical clinical data creation. In this paper, we provide an overview of two typical methods: the natural language-based method (also known as symbolic text processor, or SymText [5,11,12], and the clinical model-based method (also known as openEHR) [10,13].
1) Natural language-based method
Natural language processing (NLP) allows a machine to be able to read and learn text [11,12]. Methods based on NLP to extract information from EHRs have been proposed [4-6]. SymText, which is proposed Koehler [5], is one of them. The purpose of SymText is to construct structured data that enables diagnostic systems to be used for medical decision making and alerting systems.
However SymText improvements are still needed in lexicon, grammar, and transformation. Presently, SymText is not accurate enough, especially on unclear reports, to be used to automatically generate the characteristics.
2) Clinical model-based
An archetype is a re-usable, formal model of a domain concept. Archetypes are used to create detailed clinical models of for example observations like blood pressure or a specific laboratory results, information related to the evaluation of a clinical problem, related to activities like prescribing of medications etc.
The openEHR templates are used to adjust and combine archetypes for specific use cases and local needs. Templates are connected to entry forms (documentation templates), and may be bound to terminologies [14].
The purpose of overall researches and tools is to develop structured data set in some specific medical fields. According to the need, we propose an X-ray observation entry program which is possible to interlock with EMR and PACS. Moreover, using the proposed system, observational mistakes can be reduced because the system consists of radio button type and/or structured type entry system. Sometimes, even clinical experts can err in reading text without considering the characteristics of some diseases. However, the proposed system provides the two entry routes for various diseases, which reduces mistakes. Furthermore, the system is applicable to construction of a data mart for clinical research, health information exchange, and constructing content-based system, and etc.
2. Description of Chest X-ray Entry System
Medical record is a document of a patient's medical history that contains diagnosis information, results of treatments, laboratory results, and radiology report, among other information. The typical elements of medical records of D hospital in Daegu city are listed in Figure 1.
However, current EMRs have different types of architectures and terminologies that vary from one hospital to another. Therefore, exchange of data is onerous, given the lack of standardization. Moreover, observation reports for medical radiology images such as X-ray, CT, and MRI are typically written in a narrative way, which is different from laboratory results, as shown in Figure 2.
Laboratory results are presented in a way that is readily interpretable by clinicians, and can be directly stored as a computer file (Figure 2). However, in case of an observation report for radiology, such direct conversion to a computer file is onerous, if not impossible, and data exchange is hobbled by the free text form of the information.
Presently, we propose a simple chest X-ray entry system. The system process is diagrammed in Figure 3.
Firstly, chest X-ray images according to patients are transferred into the chest X-ray observation data mart through the conversion interface. Secondly, clinical experts check the chest X-ray on-line using the proposed entry system through on-line, and the checked image is stored with the observation results. Searching for the data of a specific patient is possible using an identifier such as patient number and/or patient name. Moreover the proposed chest X-ray entry system has various applicable fields such as data mart composition, health record exchange, and other contents-based systems (Figure 4).
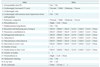
We designed chest X-ray observation indexes based on consultations with clinical experts. Significant and frequently occurring indexes were selected, and the values of input options were designed with items that would be recognizable to clinicians (Table 1). Parts 3, 14, 16, and 20 are the short narrative parts. In part 3, the real value of cardiothoracic ratio, which is used to diagnosis cardiomegaly, is inputted. Parts 14 and 16 are where the observed number of masses and nodules, respectively, are entered. Part 20 is for the input of any comments. To specify the regions where unusual states exist, the chest region was divided into seven parts, as shown in from indexes 8-13 and 15. In the indexes, RULF, RMLF, RLLF, LULF, LMLF, and LLLF stand for right upper lung field, right middle lung field, right low lung field, left upper lung field, left middle lung field, and left low lung field, respectively.
III. Results
In this section, we show configuration of the implemented system. The implemented chest X-ray entry system consists of five parts as shown in Figure 5.
The configurated implemented chest X-ray entry system consists of five parts (Figure 5). ① represents the information of patients such as patient number, name, and sex. ② shows the list of the chest X-ray images according to patients. ③ shows the diagnosis indexes and input options. ④ represents the image selected in part ②. ⑤ is the main menu. Using the sub-menus of part ⑤, it is possible to edit the index and input options, to extract observation result as excel format, and to search specific patient's chest X-ray with result. Figure 6 shows an example of a search result for one patient.
Based on the Table 1, we have implemented detail indexes and input options as shown in Figure 7. Parts ①, ②, ③, and ④ are narrative parts. In case of part ①, the diagnostic criteria could differ according to clinical experts. Therefore, we made the free-text part to clarify the ratio of cardiothoracic ratio (CTR), which is used in the diagnosis. Moreover, if any other comments exist for the given chest X-ray image, the clinical expert(s) can write the extra comments in index 19 by selecting the "Any" option.
To verify the observation results, it is possible to save the observation results in an Excel format. The example of a result is shown in Figure 8. From Figure 8, ① shows basic information of patient such as patient number, name, sex, and age. Part ② represents the diagnosis indexes. In part ②, we have added the explanation for part ③. In the results part, the selected options are represented, not as words, but as numbers, because it is easy to use numerals in analyses to analysis. However, it is possible to return the selected options to words if necessary.
Although the proposed chest X-ray observation entry system is convenient and can be used in various applications, the proposed system is limited to chest X-rays. Moreover, it is as yet unable to interpret semantic information. Therefore, to improve the quality and applicability of system, more research on techniques such as X-ray, CT, and MRI of the abdomen is required.
IV. Discussion
Although various other medical imaging techniques have been proposed, such as CT, MRI, and positron emission tomography, the X-ray (especially the chest X-ray) is the most common and widely used examination method in medicine. Especially, chest X-ray, which is used to evaluate normality of organs inside chest such as lungs, heart, bones, and etc., is one of them. The development of PACS and EMR systems has spurred interest in the exchange of medical records between medical centers. However, the free text format of most medical reports hinders this goal. Therefore, to extract medical information automatically from the reports, various methods based on natural language processing have been proposed. In other cases, to create encoded and structured data, studies examining clinical content have been undertaken. However, the techniques are rudimentary and remain difficult to use by clinical experts and/or need to improve in various cases.
Therefore, in this study, we have proposed a chest X-ray observation entry system that can be interlocked with hospital EMR and PACS systems. Using the entry system, we were able to collect data in a simplified and standardized form. Moreover, the proposed system is useful in constructing data marts that are large enough to interlock with EMR and PACS systems. Another advantage of the proposed entry system is its ability to reduce mistakes while checking the chest X-ray. In some cases, clinical experts can make a diagnosis without due attention to X-ray findings. However, because the proposed system shows representative lists for diagnosis, such a mistake could be reduced. Moreover, because the proposed entry system consists of radio buttons according to indexes, it is convenient and user-friendly.
Nonetheless of the advantage of the proposed entry system, it is limited to interpret semantic information from the observation results. Therefore the expended researches based on the entry system in various other fields are required to extract semantic information.








 XML Download
XML Download