

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Medical records, including all data such as electronic media and images, assists medical diagnosis for checkup and patient measurement, and ensures continuity of treatment [1]. This record, with its sensitive information on a patient, must be handled carefully to avoid any damage due to external exposure leading to violation of privacy, psychological/social/economical/legal disadvantage and misuse of information [2]. Therefore, the majority of nations regulates by law the careful management of all such information included in the medical record. In Korea, the Medical Law strictly restricts the use except cases needed by a doctor for treatment of a patient (Article 21 of the Law).
Recently, there are increasing cases of treatment information record being read, copied and taken out of the medical institution for secondary use such as insurance or request for payment, legal use due to increased number of medical disputes, as well as use for treatment such as follow-up treatment at the other medical institution. This increasing demand and frequency in the use of medical information can increase the chance of misuse of patient information, including medical record. Especially, with the increase in frequency in the use of medical information in the digital age, the patient privacy is endangered [3], and various leakages of information against the will of the patient have been reported [4]. With the increase in the field of use and necessity of medical information, the necessity of new guides and principles related with the superintendence and regulation of medical records and medical information are being issued.
For example, the Health Insurance Portability and Accountability Act (HIPAA) of the US actively prescribes the right of reading self-information as part of the right-to-know of the subject of information. It is therefore prescribed that the patient, the subject of information as a possessor of the right of claim on the institute holding self-information (system manager) to read self-information (the right of access to self-information) can claim for reading self-information, and the institute should permit reading unless of due reasons. It also is clarified that a copy which the subject of information can be understood is to be prepared and delivered in case self-information is recorded in film, magnetic tape, or magnetic disc, other than in document. This law not only ensures the right of the subject of information on health-care information (reading of access, correction, use details, right to be issued of a copy), as well as imposing a duty of safety management of information on insurance beneficial institute (Health Plan), but also mandates a prepared detailed regulation to be able to settle various problems occurring in using and handling medical record information, thereby backing the use [5]. HIPAA functions as a guideline for active use of medical information as well as being a powerful means of regulating privacy [6], thereby reducing the possible occurrences of problem by the smooth use of the relevant medical information.
In Korea, according to up-to-date authoritative interpretation of Ministry for Health, Welfare and Family Affairs on this matter (enforced in September 2003), it is prescribed that reading and copying of medical record is to be provided to fulfill the right-to-know of a patient, and the character and authorization of the mandator and the one being mandated should be clarified in detail through a letter of attorney of a patient when reading a medical record or issuing a copy is requested by a third party to prevent misuse, and certificate of seal impression or ID which can prove this objectively. And, if a legal act is limited in the case that the patient is minor or incompetent, a civil person in parental authority on behalf of the patient can authorize necessary matters to an attorney, and reading medical record, issuing copy or diagnosis, etc. can be included according to authorization by authoritative interpretation taking measures in issuing medical record and a copy. But, the medical service providers of medical institutions under the regulations should exactly know the standard regulating the opening of medical information that can distinguish an individual to observe effective procedure, laws and regulations, vocational ethics, and standard of approval, and exactly know whether there is a conflicting law and the required documents to be submitted in permitting the use. This also corresponds with the case of a patient and the acting patient requesting for the issue of a copy of the medical record. It is doubtful that the problem has been settled through these bylaws, and that each hospital in case of lack of supporting evidence in accordance with custom. So, medical record management department has been carrying out access, opening and complementary management of treatment information on the request for issue of a copy of a medical record of inner user and outer user under operative law. However, is presumed to be handling by the bylaw, but is actually handling according to the bylaw of each hospital in accordance with their internal custom [7,8].
Only recently has any study been conducted to survey the recognition of security issues on medical information and confidentiality of private information of patients and the general population [2,9]. Furthermore, no survey has examined the management related with the issuance of a copy at a medical institution which is the official and most frequent path via which the leakage of medical documents occurs out of medical institute.
Therefore, this study was conducted for one year during the calendar year of 2007 at 5 tertiary referral hospitals over the country to analyze the present condition that a copy was issued when the documents required in issuing a copy of the medical record in authoritative interpretation of Ministry of Health and Welfare had not been prepared. I also examined the factors related to the unpreparedness of the required documents to present the basic data to improve the management of medical information.
II. Methods
1. Subjects of Research and Data Collection Method
The study subjects were 7,296 persons (cases) corresponding to the number of the copies of medical documents issued for 1 year from July 1, 2007 to June 30, 2008 at 5 tertiary medical care institutions over the country. From each region of Seoul, Gyeonggi, Yeongnam, Chungcheong, and Honam (including Jeju) one tertiary referral hospital was selected as a good representative of the utilization of medical information as central institute treating serious cases and considering of possibility of cooperation.
With the cooperation of the heads of the medical record management departments at the 5 selected hospitals, the database on total issuance for one year was extracted into Excel data in structured form, and a joint database was constructed with the data from the 5 hospitals.
2. Principle Research Variables
The dependent variable was whether the required documents were fully prepared or not when requested for issuing copy of medical record. This dependent variable was generated using information of constructed database, and was used in the analysis. That is, 1) case of one requesting the issue of copy is the applicant himself having some identification; 2) case of one other than who requested the issue of copy (spouse, child, brother, relative, 3rd party, insurance company, etc.), ① case of the subject of issue is an adult, and the case of identification of an applicant and letter of attorney and certificate of seal impression of subject or legal representative were presented, ② case of the subject of issue was a minority, and case of identification and documentary evidence on family relations (one among copy of resident registration, certificate of health insurance, copy of family register) were presented is defined as such that the required documents are fully prepared, and the case of not being able to satisfy this requirement is defined as unpreparedness of the required documents.
The factors related to whether the required documents are fully prepared or not are the demographic characteristics of the subject of issue, medical use characteristics of the subject of issue, and characteristics related with the issue of copy. The variables in detail are as follows. First, gender, age, residential area, and type of coverage are included in the demographic characteristics of the subject of issue. Residential area among these is reclassified as residential area and residential region using 6 digits of the zip code before amendment notice in August 2008 in the database, and used in this research. Next, the variables used in the analysis of the medical use characteristic of the subject of issue are channel of issuance (outpatient, in hospital, emergency), used consultation subject, issuance hospital, and location of hospital. Lastly, the characteristics related with the issue of copy are applicant of issue of copy himself, family (spouse, child/parent, brother), private insurance company, other (relative, 3rd party, other are reclassified as other), use of copy, number of issues, cost of issuance and type of issued copy (outpatient record, inpatient record, emergency record, doctor record, surgery record, nursing record, clinical pathology, image inspection).
3. Analysis Method
The data of each hospital were inputted in one data file using MS Excel, and analyzed using SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA) statistics package after examination of errors and correcting process. The analysis method used in the analysis was as follows.
The characteristic distribution, association of characteristics and unpreparedness of documents were analyzed using chi-square test. Finally, a multiple logistic regression model was constructed by using the variables related in the significance level (p < 0.05 level) with the unpreparedness of the required documents as a result of the chi-square test to examine the factors influencing the unpreparedness of the required documents.
III. Results
1. Distribution of Characteristics of the Research Subject and Relation with Unpreparedness of the Required Documents
1) Distribution of demographic characteristics and relation with unpreparedness of the required documents
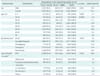
The fully prepared documents were 6,212 cases (85.1%) and the unprepared documents were 1,084 cases (14.9%). Demographic characteristic distribution of the subjects showed 52.9% males compared to 47.1% females, and in age, 1,496 were in their 50s (20.5%), the highest, and 412 were in their 10s (5.6%), the lowest. In residential regions, Seoul region was 9.6%, Gangwon/Incheon/Gyeonggi region was 32.0%, Daejeon/Chungnam/Chungbuk region was 11.8%, Busan/Gyeongnam/Daegu/Gyeongbuk region was 19.9%, and Gwangju/Jeonnam/Jeonbuk/Jeju region was 26.6%. According to the type of medical security, National Health Insurance (NHI) was the most at 89.6%, followed by medical aid at 3.4%, occupational health and safety insurance at 1.6%, car insurance at 1.4%, patients with no insurance at 2.0%, and other at 1.9%. As the unprepared documents seen by gender, unprepared documents of males was 15.7%, which was significantly higher than that of females at 13.9% (p = 0.041). By age in unprepared documents, those in their 70s was 35.9%, highest, and in their 30s was 8.7%, lowest, and the difference was statistically significant (p = 0.000). By residential region in unprepared documents, residents of Busan/Gyeongnam/Daegu/Gyeongbuk region was 19.0%, highest, and residents of Daejoen/Chungnam/Chungbuk region was 8.2%, lowest, and the difference was statistically significant (p = 0.000). According to the type of medical security in unprepared, general patient was 22.4%, highest, and medical insurance was 14.4%, lowest, and the difference was statistically significant (p = 0.016) (Table 1).
2) Distribution of the variables related to medical utilization and association with unpreparedness of the required documents
Medical use characteristic distribution of the subjects by issuance channel of copy showed that 75.5% was issued at the outpatient department, 23.2% in hospital, and 1.4% in the emergency room. Internal department (3,097 persons, 42.4%) and surgical department (3,093 persons, 42.4%) were the departments mostly used, and other departments with 303 persons (4.2%) was the least. By the issued hospital, "D" hospital was 2,220 persons (30.4%) having the most, and 'A' hospital was 971 persons (13.3%) having the least. The case the hospital being located in the residential area was 74.9%, which was higher than the case of out of the residential area at 25.1%. The unpreparedness of the required documents by issuance channel showed 27.4% for the unprepared document in the case of issuing 'in hospital' was significantly higher than 11.0% of 'outpatient' and 16.0% of 'emergency room' (p = 0.000). By the department used, the document unprepared in use of the internal department was the highest at 16.7%, and the pediatrics was the least at 5.6%, and the unpreparedness of the required documents was statistically significant (p = 0.000). By the issuance hospital, unpreparedness of the required documents of the users of 'B' hospital was the highest at 19.4%, and 'A' hospital was the least at 7.3%, and the difference of unpreparedness of the required hospital was statistically significant (p = 0.000). By the location of the hospital, unpreparedness was 17.0% in the case of the hospital located out of the residential area, which was significantly higher than 14.2% for in the residential area (p = 0.005) (Table 2).
3) Distribution copy issue characteristics and association with unpreparedness of the required documents
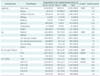
The copy issue characteristic distribution of the subjects showed that the applicant himself was 4,324 persons (59.3%), highest, and by the use for issue of copy, submit to an insurance company was the highest with 3,894 persons (53.4%) and for military affairs was the least with 263 persons (3.6%). Under 5 sheets was the highest with 3,966 persons (54.4%) in number of issues, 2.56-3.40 USD was the highest with 2,172 persons (30.6%), and more than 8.51 USD was the least with 398 persons (5.6%). By the applicant, unpreparedness of the required documents in the case of the relative was the highest at 89.5%, and the difference of unpreparedness of the required documents by applicant was statistically significant (p = 0.000). By copy issue year, unpreparedness of 'others' was the highest at 23.7%, and National Pension and private custody was the least with 11.4%, and the difference of unpreparedness of the required documents by use was statistically significant (p = 0.000). Unpreparedness of the required documents of more than 51 was the highest at 24% by the number of issues, and by issue cost, more than 8.51 USD was the highest at 22.1%, and the difference of unpreparedness of required documents according to issue number and issue cost was statistically significant (p = 0.000) (Table 3).
4) Distribution of type of issue document and association with unpreparedness of the required documents
In the characteristic distribution of the type of issue document of the subjects, outpatient record, inpatient record, and doctor record were the characteristic variables having applications more than non-application, and there were more non-applications than applications with the remaining variable. As a result of analyzing the relation of distribution of type of issue document in relation with issue of copy and unpreparedness of the required documents, the outpatient record by the characteristic variable (p = 0.000), inpatient record (p = 0.000), doctor record (p = 0.001), nursing record (p = 0.019), and image test (p = 0.007) were statistically significant (Table 4).
2. Factors Influencing Unpreparedness of Required Documents
As a result of multiple logistics regression, the difference of unpreparedness of the required documents of all age categories was significantly higher compared to below 10-year-old in the case of the age of the patient, and the odds ratio (OR) of more than 70-year-old was the highest at 149.240 (95% confidence interval [CI], 75.926 to 293.345). The difference of unpreparedness of the required documents in all areas based on Seoul by the residential regions was low, but was statistically significant. However, the OR of Gwangju/Jeonnam/Jeonbuk/Jeju region was 0.096 (95% CI, 0.028 to 0.327), which was significantly lower than the Seoul region. As issuance channel, the unpreparedness of the required documents document was significantly higher in the case of 'in hospital' than in the case of application for issue through 'outpatient' (OR, 13.325; 95% CI, 9.562 to 18.567), and the occurrence of unpreparedness at the boundary level in the case of application in an emergency room was higher (OR, 2.753; 95% CI, 0.905 to 8.369). In the case of the department used, only obstetrics and gynecology (OR, 0.408; 95% CI, 0.178 to 0.942) had significantly low unpreparedness, there was no significant difference in the remaining departments based on internal department. By the hospital, unpreparedness of the required documents of 'B' (OR, 0.086; 95% CI, 0.020 to 0.366) and 'E' (OR, 0.128; 95% CI, 0.035 to 0.466) Hospitals were significantly lower, and there was no significant difference with the remaining hospitals based on 'A' hospital. Based of the applicant himself applying for issue of copy, unpreparedness was higher in the case of spouse (OR, 1199.411; 95% CI, 693.547 to 2074.245), child (parent) (OR, 777.200; 95% CI, 476.758 to 1266.975), siblings (OR, 337.438; 95% CI, 50.199 to 2268.264), relatives (OR, 61341.256; 95% CI, 8036.421 to 468,212.138), and others (3rd party) (OR, 2018.290; 95% CI, 1007.020 to 4045.096), but unpreparedness of private insurance company (OR, 0.249; 95% CI, 0.104 to 0.595) was only significantly lower. In the case of use for issuing copy, unpreparedness was significantly higher at the border level for military affair (OR, 2.025; 95% CI, 0.889 to 4.613), based on one to submit to the other hospital, but unpreparedness was significantly lower in case of one for insurance company (OR, 1.567; 95% CI, 1.128 to 2.177), one to submit Corporation of National Pension (OR, 0.362; 95% CI, 0.182 to 0.719). Unpreparedness of the required documents was significantly lower (OR, 0.430; 95% CI, 0.189 to 0.975) statistically in issuing copy of more than 50 sheets based on five issues, and unpreparedness of the required documents was significantly lower (OR, 0.389; 95% CI, 0.222 to 0.682) on 2.56 USD-3.40 USD on the basis of 0.85 USD for issue cost. The factor of unpreparedness the required documents in issuing a copy by residential area was that unpreparedness of the required documents was significantly higher based on the non-issue of relevant residential area (OR, 2.171; 95% CI, 1.550 to 3.040). Unpreparedness of the required documents by all residential areas had no significant difference (Table 5).
IV. Discussion
1. Discussion on Research Method
The research data were collected from 5 tertiary medical institutions in 5 different provinces. To minimize the influence by local variation or seasonal variation, the nation was divided into 5 regions with 1 tertiary medical institution being selected from each region, and the data were collected for one year. However, these 5 medical institutions may not be good representatives of all medical institutions of Korea. Though the main issuer of copies of medical record is the tertiary medical institution, there are many hospitals and clinics, and number of copies issued from these institutions should be no less than tertiary medical care institutions. In addition, the practice of issuing copies of such medical institutions may be different with the tertiary medical institutions judged to be higher in level of procedural rationality. Therefore, the data may not be representatives of the related laws or guidelines in time of issue of copy. However, the study results may be adequately used as evidence.
As this research used data of the constructed subject of issuing copy, it was limited due to the lack of many variables. Especially, the social anthropological characteristic variables necessary for viewing the relevant factors and subjective recognition factor variables, such as satisfaction and dissatisfaction in concrete and in three dimensions, could not be included. In addition, the experience and opinions of the staff in charge and the specialists working in issue of copy that is necessary for drawing proposal on improvement of the system were not included.
One of the most important problems in relation with the research method was the measurement of the dependent variable. This research was limited to the cases where the copy had already been issued, and the full preparation of the required documents had been defined and calculated. Therefore, the case issue in which unprepared documents were rejected at the point of application for issue had to be excluded from this research. Further research using data at the point of application will be necessary to determine the scale and actual condition of the problem between the applicant and the person in charge of issue. Therefore, the actual condition of the slackening of the applying directive could be clearly determined by computing the issuing rate with the unprepared at the point of application for issue on denominator. Separate data are necessary for this. Nevertheless, the merit of this research is that it is the first in this area and was carried out using large-scale data. Therefore, the study results could be applied as the foundation of research in this field, and improved research based on the present study results.
2. Discussion on the Research Results
This study was conducted by analyzing the results of logistics regression according to the related factors and by postulating the possible causes to explain these results in the absence of any related precedent study.
As a result of the multiple logistics regression analysis, the factors independently influencing the unpreparedness of the required documents were the patient age, issuance channel, treatment department, treatment hospital, residential district, applicant of issue, and inpatient record among the type of medical record. Each of these factors is discussed below.
Regarding the patient age, unpreparedness of all age category divided at 10-year intervals was significantly higher compared to below the age of 10. For the reason why unpreparedness of below the age of 10 was lowest, we presumed that their parents applied issue as agent of them and because of their high concern for children' affairs they strictly prepared relevant documents. The tendency of unpreparedness increased with increasing age to a maximum for the patients over 70-year-old. The probability of unpreparedness was judged to be increased for the elderly due to poor ability to recognize, low familiarity with related information, and higher probability of preferring informal relation rather than formal relation in cases related with the applicant himself. However, by focusing on the examples issued in a hospital, the probability of the hospital being more permissive in applying a guide on elderly patients could have been applied.
Related with the high unpreparedness of the relevant documents for those in parental authority or authorized in age groups of under 19-year-old and more than 65-year-old, the following cases correspond to that a particular case experienced by the present researcher who was in charge of managing medical reports and issuing copies. For example, there were many cases of an inability to confirm the identity when the guardian of pediatric patients who had received treatment that day requested issue of copy. Many patients and guardians did not have medical insurance cards or other identification with them in visiting medical institution after medical insurance card being computerized. Especially, there were many cases of grandfather or maternal grandfather instead of parent coming to the medical institution for pediatric patients, and there were cases such as a change of family relation like cohabitation, divorce, living separately that increased the difficulty in confirming the identity due to the change of legal qualification, requesting for a copy of the medical record of a child under age not living together after divorce, and requesting issue of copy with the copy of resident registration before divorce of a mentally retarded spouse as evident. Cases such as requesting a copy of medical report of cohabitant in de facto relationships could be included in such examples. The majority of medical institutions notify in detail on the procedure of issuing copy and the required document through their homepage because such cases occur frequently. Nevertheless, they still experience cases of requesting of issue without preparation of related documents. Although this could be considered a problem of an applicant for issue of copy not checking, it remains a common case for those working in related fields that there are many cases of issuing copy with an abbreviated procedure of confirming document so as not to trouble the applicant at private medical institutions. Those in charge of issuing copy frequently experience such situations that contravene the related directive from the Ministry of Health and Welfare. The problem of proving the identity of the guardian for a person under the age of 19 is expected to be gradually improved through increased publicity, but there remain cases that are difficult to settle in such way. The case of an elderly person not having a certificate of seal impression is typical. In such a case, authorization through certificate of seal impression may not be possible, or may need frustrating procedure that take a long time in urgent situation. In such special cases, examples of violating the directive are increasing in order to avoid troubles with customers. In such cases, medical institutions confirmed the identity by various methods. The doctor certifying an identification of a patient or a nurse confirming the patient or guardian based on recognition in process of nursing are typical examples. As a result of this research, although identifications were confirmed using routine means or with internal directives in the case of unprepared documents, most of these cases were presumed to lack documents.
Thus, it is necessary to improve consciousness of people on such as spread of recognition that corresponding responsibility follows on exercising the right to self-decision using and controlling medical information. And the medical institution notifies to check it's homepage on issuing copy before applying, and any special measures that need to be prepared for a patient or guardian having difficulty in following such means.
The partially amended legislative bill of the medical law in December, 2008 has clarified the incomplete section of the existing law on reading the patient treatment records. Compared with the existing medical law, this legislative bill restricts the reading of the record to only the patient himself, spouse of the patient, ascendant/descendant in a direct line, or ascendant in a direct line of the spouse having written consent of the patient and certification showing family relations, and allows the application for reading and issuing copy on only the 'Code of Criminal Procedure/Code of Civil Procedure/National Health Insurance Law/Medical Aid Law/Workmen's Accident Compensation Law/Automobile Third Party Liability Law/Military Service Law/Law on School Accident Prevention and Compensation/Law on Defoliant Aftereffect Patient Support.' Nevertheless, similar illegal examples will likely arise after revision of the law. Therefore, it is necessary to formulate guidelines based on real situation. Joint work between the academic society and the related government departments is recommendable.
In case of issuance channel, unpreparedness of the required documents document was 13.3 times higher when the issue was requested 'in hospital' than when requested through the outpatient clinic. This was attributed to the greater ease in confirming a patient through various channels in the hospital.
Regarding the treatment department, obstetrics and gynecology was significantly lower than internal departments, which was attributed to the higher possibility of problems caused by the application of a stricter standard.
Regarding the treatment hospital, the unpreparedness of 'B' and 'E' hospitals was significantly lower than that of 'A' hospital. In the case of 'E' hospital among them, as a public hospital, it was possible to have a organizational culture to obey standard protocol related with issuing .
Regarding the residential area of applicant for issue with Seoul as the standard group, the differential rate of Gwangju/Jeonnam/Jeonbuk/Jeju was very low at 0.1. In the case of Jeju area that was island, this was attributed to be strictly prepared by considering that all 5 hospitals were in inland. But, in the case of Honam area, the possibility of a local hospital such as 'E' hospital applying a strict directive, resulting in discrimination in this area, could not be excluded.
Regarding the application subjects, all subjects except insurance companies were significantly higher in unpreparedness compared to the applicant himself. On bivariate analysis, the completion rate of the required documents in the case of the applicant himself was 95.9%, compared to the completion rate of insurance companies. This high completion rate was attributed to the absence of any identification requirement through documents, which simplified the required documents compared to other subjects of application. On the contrary, cases other than the applicant himself were attributed to the requirement to prepare more documents other than identification. The differential rate was especially high in spouse, relative, and third party, suggesting that the related directive was simplified for confirming the identity by means other than documents in the case of a patient applicant for issue of kinship. However, this needs to be examined carefully because there are many cases of documents unprepared in the case of third party. This suggests the necessity of preparing a particular guide in this area and of firmly establishing strict application criteria. However, the unpreparedness of the required documents was significantly the lowest compared to self application in the case of insurance companies with a total of 6 cases in a year. This was attributed to the fact that the insurance company as an applicant for issue knows the related laws well and is likely to thoroughly prepare related documents, and the medical institution has stricter standards on demand of this subject of application. In other research related to this [9], the response of the subjects in a survey related with whether to open actual data of personal treatment managed by National Health Insurance Corporation to the question, 'Is it better for the private insurance company to provide personal disease information so as to reduce insurance fraud and thus reduced the insurance bill of health insurance product?', 38.3% of the respondents answered positively, and 33.3% negatively, and the difference in the response exceeded the error tolerance (3.1%). This result was attributed to the presumption that this situation was beneficial to oneself. On the question, "Do you agree with the National Health Insurance Corporation providing personal disease information to private insurance companies?" without assuming specific situation, 70.5% opposed, and only 25.7% agreed. The question of whether to provide disease information to private insurance companies is controversial worldwide due to the opposing interests of these companies and the patients, even as private insurance companies set high demands on treatment information of the patients. Nevertheless, 'absolutely disapproval' is the general principle taken by each nation except the US where the combination of insurance company and medical institute such as managed care is permitted [9]. Considering this, it is necessary to control thoroughly medical record and for people to recognize that necessity.
Regarding the use of issue, unpreparedness was higher for submissions to insurance company and National Pension Corporation compared to for submit to other hospital for treatment. This suggests that a smoothed standard rather than a strict standard was applied, and therefore that adequate relevant measures need to be prepared.
The number of issues was also the independent related factor, and the unpreparedness of the required documents of more than 51 sheets was significantly lower than that of those under 5. The necessity of more copies meant higher possibility of being related to legal dispute such as lawsuit, which were attribute to the subject of application for issue thoroughly prepares documents, and the stricter standards and guides applied by medical institutions. Regarding the cost, unpreparedness of the required documents with 2.56 USD to 3.40 USD was significantly lower than that under 0.85 USD (the cost to issue 1 copy varied among the five hospitals), which supports the above assumption.
Finally, unpreparedness of the required documents for in-hospital record among the original records was significantly higher compared to that for other documents. This was attributed to the compensating channel, which suggests that it is not a case of applying for issue documents related to the hospital. So, in the case of having in-hospital register, the patient living long at the medical institution may have been acquainted with the hospital staff, which simplified the procedure. In addition, a tolerant guide may have been applied to in-patient cases, considering that most of admission cases had came from more far from hospital than outpatient or emergent treatment.
The study results revealed that the medical records recorded by the medical institutions are used not just to facilitate communication between doctors in and out of the medical institution for treatment, but also at various other places with various purposes, and that copies are issued according to various requests. The hospital association sponsored by the Ministry for Health, Welfare and Family Affairs voluntarily publishes a guide for issuing copy to protect health information, but the documents required for third party or authorization are often not prepared by the applicants, and the medical institution issues the copy by confirming the identity through other channels if the submitted documents are lacking. So, it was clear that, at least on documents, the medical information of patient was managed in dangerous level. But, as a result of assumption considering customary issuing practice and checking the reason for such result directly through a person in charge and, we concluded that most of the hospitals were managing their procedure issuing medical records based on the principle. The results suggested that the hospitals interpreted the law flexibly for the convenience of their users as 'customers' within the permissible range in Korea. Thus, the efforts of hospitals to observe the relevant regulations should be carried out by clearly regulating authoritative interpretation not to have room for dispute.
The collective study results support the necessity of confirming the method and guidelines for confirming the consent required in the common copy issuing procedures in the case of treatment at other hospitals and for patients in hospital. So, when the person in question actually cannot authorize, or cannot prepare documents for authorization, a procedure is necessary that reflects the actual experience and customs, rather than the strict and regulated procedure. This is more necessary due to the difficulty in accurately reflecting all the aforementioned legal matters. It is possible by preparation of standardized realistic guide that widely accepted experience and customs of hospitals. And relevant academic society may make a role for this.
The results highlight the need for greater social effort to improve the level of recognition on health medical information of the people. I hope that this research meaningfully contributes to the start of such effort.
Regardless of the field, the reason why, with expending high cost, private information is preserved and managed is due to the necessity of that use. However, the use of such information holds the danger of violation of private life and human rights. In the health field, intimidation could be more serious, so the basic health law regulates 'confidentiality' as one of the human rights on health (Article 13). So, it is clear that this case is handled as the factor of fundamental rights. The leaking of any information without proper reason by the person in charge of handling and managing such information is punished severely, with both criminally and professional sanctions, and severe regulation is applied in all nations with similar health system to Korea's such as Germany, France, and Taiwan [9].
With the increasing complexity of modern society, and the corresponding expansion in the amount of medical information and scope of use, various stake-holders are competing with each other for access rights to personal information. Therefore, the dangers associated with complications arising from improper utilization of information and privacy protection are increasing. Therefore, very 'delicate and elaborate approach' is required for maintaining both 'effective utilization' and 'privacy protection' [10-12].
Health information, including personal information produced in the process of patient treatment, is preserved and managed in the form of medical records. The issuance of medical records from medical institutions occurs via copies of the record in most nations including Korea. The danger of the leakage or misuse of patient medical records in the digital era is rapidly increasing, so management has discussed the concern over the access for the circulation of electronic documents. Although the management of electronic information is strictly limited, the media a copy of medical record in form of document which circulation of information increase is not. So, although the related laws and authoritative interpretations exist, 'delicate and elaborate access' has not been reached to settle examples in detail caused by conflict of used information. This demands more than the strict application in consistent and standardized form of the related authoritative interpretations and guidelines. So, the regulation must have feasibility and reality that can be applied to most of various examples occurring and able to occur as well as be clear without any confusion. Colliding with actual operation process, law and guide could be treated lightly or ruined, thereby preventing the law and guidelines from accomplishing genuine legislative purpose. Therefore, it is judged to be the urgently demanded theme for preparation of improved solution to study actual condition and relative factor of legal document requirement problem with situation related with issuing copy which groping of solving method was hard for not having organized research/organization though concerned staffs experience.



 XML Download
XML Download