

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Menopause is a natural part of physiological aging in women.1) Surgical early menopause occurs when a woman begins menopause due to medical reasons instead of the natural aging process. The incidence of cardiovascular disease is lower in premenopausal women and increases after the onset of menopause, and this increase is more pronounced after surgical menopause.1)2) Cardiovascular changes are often asymptomatic during the menopausal transition, and there is an association between the onset of menopausal transition and the rate of advance of atherosclerosis.2)3) However, women with surgical menopause do not experience a premenopausal transition period, and this negatively impacts many organ systems, including the cardiovascular system.2)3)
The causes of atrial fibrillation (AF) are multifactorial and include inflammation, oxidative stress, genetic and environmental factors, and atherosclerosis risk factors, all of which can also impact the pathogenesis of AF.4)5) Although many studies have suggested that menopausal and atherosclerotic heart diseases and myocardial infarction increase in such cases, there are different results regarding the development of AF and the increased risk.6) Additionally, some methods have been developed to predict AF early.
Atrial electromechanical conduction duration is a feature that represents the functional and electrical integrity of atrial cells.7) Electromechanical abnormalities originating from intra-atrial and inter-atrial transmission disturbances are associated with an increased risk of AF.4)5)8)9)10)11)12) Atrial electromechanical delay (AEMD) is evaluated by tissue Doppler echocardiography, and an increase in AEMD duration was determined to be an independent risk factor for AF development.4)5)8)9)10)11)12) Left atrial (LA) volumes may also be used as a measurement of atrial function and health. Increased LA volume and diameter are associated with cardiovascular pathologies and are risk factors for AF development. Atrial volume overload, also assessed using echocardiography, results in atrial myocyte damage and affects mechanical functions.4)5)8)9)10)11)12)
In this study, we evaluated the AEMD by tissue Doppler echocardiography and LA mechanical functions by volumetric echocardiography in surgical early menopause patients and healthy controls.
METHODS
Study protocol
The study included 33 patients with surgical early menopause and 29 control subjects matched for clinical and demographic characteristics. We excluded 4 patients in the surgical early menopause group due to the presence of AF with valvular disease. All participants signed a consent form following the receipt of study information. Patient age, sex, body weight, height, cardiovascular risk factors, current medications, and history of other systemic diseases were recorded in the patient form. The duration and cause of surgical menopause were also recorded. The median time since surgical operation was 2.1 years (range, 1-5 years). Individuals that had had surgery 1-5 years prior to the study were included.
The exclusion criteria included surgical menopause for less than one year, being on estrogen replacement therapy, improper measurement of blood pressure, history of coronary artery disease, heart failure with preserved or reduced ejection fraction (EF), cardiomyopathy, severe valvular heart disease, poor echocardiographic image quality, and presence of AF or history of paroxysmal AF attack. The protocol was approved by the institutional review board of the Faculty of Medicine, Ondokuz Mayis University and adhered to the Declaration of Helsinki.
Standard echocardiography
The echocardiography was performed on each patient in the left lateral decubitus position through the parasternal and apical windows. M-mode, two-dimensional, pulsed and color flow Doppler echocardiographic imaging of all patients was performed by the same operator using a Vivid 7 device (3.5-MHz phased array transducer; GE Medical System, Horten, Norway). Posterior wall thickness, interventricular septum thickness, left ventricular end-diastolic diameter, left ventricular end-systolic diameter, and LA anteroposterior diameter were measured using the M-mode technique. The modified Simpson technique was used to measure the left ventricular EF.
Transmitral flow speeds (E and A) were assessed by pulsed wave Doppler in the apical four chamber windows. Pulsed wave tissue Doppler imaging was performed using a low-wall filter setting, a little sample size, and an ideal gain. The Doppler pulse was arranged parallel to the direction of flow. For the tissue Doppler view of the annular movement, the sample volumes were placed at the septal, lateral mitral, and lateral tricuspid annuli in the apical 4-chamber window. Peak early (e′) and late (a′) diastolic velocities and systolic velocities (s′) were calculated. At least three values for each measurement were averaged, and the data are presented as means of three to six consecutive heartbeats.
Evaluation of atrial electromechanical delay
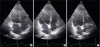
The tissue Doppler echocardiography was performed with transducer frequencies of 3.5 to 4.0 MHz by regulating the spectral pulsed Doppler signal filters until a Nyquist limit of 15 to 20 cm/s was achieved and by using the minimal ideal gain. The monitor scan velocity was adjusted to 100 mm/s. In the apical four chamber window, the pulsed Doppler sample volume was positioned at the septal annulus, the lateral mitral annulus, and the lateral tricuspid annulus. Atrial electromechanical connection (PA′), the time period from the beginning of the P wave on the superficial electrocardiogram to the beginning of the late diastolic wave (A′), was assessed for the lateral mitral annulus (PA′ lateral), septal mitral annulus (PA′ septum), and lateral tricuspid annulus (PA′ tricuspid) (Figure 1). The PA′ values from three sequential heart pulses were averaged.
Figure 1
Atrial electromechanical connection (PA′), the time period from the beginning of the P-wave on the superficial electrocardiogram to the beginning of the late diastolic wave (A′) on the tissue Doppler echocardiograph (mitral lateral annulus (A), septal annulus (B) and tricuspid lateral annulus (C)).

The difference between the PA′ lateral and the PA′ tricuspid (PA′ lateral–PA′ tricuspid) represents the inter-atrial EMD. The difference between the PA′ septum and the PA′ tricuspid (PA′ septum–PA′ tricuspid) represents the right atrial EMD. Finally, the difference between the PA′ lateral and PA′ septum (PA′ lateral–PA′ septum) represents the LA EMD.4)5)8)9)10)11)12) Intra-observer coefficients of variation for intra- and inter-atrial EMD were 2.9% and 3.8%, respectively.
Measurements of left atrial mechanical functions
An electrocardiogram was recorded during echocardiography. Measurements were taken from the three cardiac cycles by the same operator. Following the collection of data, LA volume measurements were performed by two operators simultaneously and the mean values were averaged. Conventional measurements were conducted using transthoracic echocardiography and LA size and functions were assessed. All atrial volumes were calculated using a uniplanar area–length (apical four-chamber) formula. LA borders were traced using planimetry. The borders included the walls of the LA and excluded pulmonary veins and the LA appendage. Left atrial volume index (LAVI) was calculated by dividing LA volume by body surface area of patients. Maximal LA volume (LAVmax), minimal LA volume (LAVmin), and atrial precontraction LA volume (LAVpreA) were also calculated (Figure 2).4)5)8)9)10)11)12)
Figure 2
LAVmax (A), LAVpre-A (B), and LAVmin (C) measurements were made by transthoracic echocardiography using the apical four-chamber window. LAVmax: left atrium maximal volume, LAVmin: left atrium minimum volume, LAVpre-A: left atrial precontraction volume, LV: left ventricle, RA: right atrium, RV: right ventricle.
The following formulas were used for calculating LA functions:
Statistical analysis
All data were evaluated using the SPSS (Statistical Package for Social Sciences) software for Windows 22.0 (SPSS Inc., Armonk, NY, USA). Student's t-tests were performed for independent samples based on previous clinical studies; the power of the test was found to be 80.52% when a total of at least 56 subjects were included in the study. Descriptive statistics are described by the mean ± standard deviation (min-max), the frequency distribution, and the percentage. Pearson's chi-square tests and Fisher's exact tests were used to assess categorical factors. Normally distributed parameters were analyzed using visual (histogram and probability plots) and analytical techniques (Shapiro-Wilk Test). For variables without a normal distribution, Mann-Whitney U-tests were used to compare two independent groups, and Student's t-tests were used for normally distributed parameters. Values of p < 0.05 were considered significant.
RESULTS
A total of 62 women were included in the study, 33 with early menopause due to total abdominal hysterectomy with bilateral salpingo-oophorectomy and 29 healthy controls. There were no statistically significant differences (p < 0.05) in age, body mass index, coronary artery disease risk factors, or basic laboratory parameters between women with early menopause and controls (Tables 1 and 2). Additionally, there were no significant differences in left ventricle diameter, LA diameter, or blood pressure between the two groups (Table 3).
Table 1
Baseline clinical and laboratory characteristics of the surgical menopause and control groups
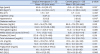
Table 2
Measurements of basic echocardiographic parameters and blood pressure of the surgical menopause and control groups

Table 3
Measurement of mitral and tricuspid leaflets annular pulse-wave Doppler parameters in the surgical menopause and control groups
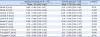
AEMD assessments, measured by tissue Doppler, are presented in Table 4. The PA′ septum (62.8 ± 12.5 ms vs. 51.1 ± 14.7 ms, p = 0.003) and PA′ tricuspid (60.1 ± 11.8 ms vs. 47.7 ± 14.5 ms, p = 0.001) were significantly higher in patients with surgical early menopause compared to controls. However, the PA′ lateral (69.6 ± 12.2 ms vs. 60.0 ± 17.3 ms, p = 0.051) was similar between the two groups. Additionally, the LA, right atrial, and inter-atrial AEMD values were not significantly altered in surgical early menopause patients compared to the controls.
Table 4
Atrial electrical activity parameters in the surgical menopause and control groups
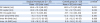
LA volumes are reported in Table 5. LAVI (28.1 ± 8.17 mL/m2 vs. 24.89 ± 7.96 mL/m2, p = 0.019), LA Vmax (49.6 ± 14.1 mL vs. 42.9 ± 16.1 mL, p = 0.004), Vmin (18.4 ± 7.0 mL vs. 15.2 ± 9.0 mL, p = 0.022), and VpreA (31.0 ± 10.9 mL vs. 24.9 ± 10.1 mL, p = 0.006) were significantly higher in patients with surgical early menopause compared to controls. However, the LA reservoir, conduit, and pumping functions and total, passive and active emptying volumes were all comparable between surgical early menopause patients and healthy controls (p = 0.09; 0.06; 0.68; 0.06; 0.48; 0.07, respectively).
Table 5
Left atrial mechanical functions in the surgical menopause and control groups
DISCUSSION
In this study, we assessed the relationship between surgical early menopause and AEMD and LA mechanical functions. We demonstrated that patients with surgical early menopause displayed prolonged AEMD and reduced LA mechanical functions compared to their healthy counterparts, although some alterations were not statistically significantly.
While women are somewhat protected against atherosclerosis during their reproductive years, this can change after the onset of menopause.13) The rate of progression of atherosclerosis increases throughout the menopausal transition, and often asymptomatic cardiovascular changes occur during the postmenopausal stage.3)13) Many pathophysiological processes are affected in atherosclerotic diseases, including changes in the LA, that contribute to the development of AF. In a population-based study, 18 different comorbidities were associated with menopause, including arrhythmia, coronary artery disease, hyperlipidemia, depression, and osteoporosis.14) Importantly, multi-morbidity decreased with estrogen replacement.14) A study by Magnani et al.15) demonstrated that menopausal age had no effect on the incidence of AF.
Following the natural onset of menopause, ovaries continue to produce androgens and other hormones1), and androgens get aromatized in the adipose tissue to produce estrogens. However, the removal of the ovaries in surgical menopause reduces this hormone production and peripheral estrogen conversion,1)2) leading to more cardiovascular effects compared to natural menopause.1)3)16) Therefore, we investigated the LA mechanical functions and AEMD, which predict AF, in surgical early menopause patients. A study by Siniscalchi et al.1) investigated the effects of surgical early menopause on cardiac arrhythmia and demonstrated that surgical menopause and estrogen replacement therapy did not significantly affect atrioventricular transmission and ventricular repolarization time in women. In a study by Dogan et al.13) Tp-e interval was significantly reduced while QT intervals and P-wave parameters were not altered in postmenopausal women compared to premenopausal women.
Inter-atrial, left atrial, and right intra-atrial AEMD durations might contribute to the onset and continuation of AF and the irregular spread of sinus pulses. These alterations are widely accepted as indications that the atrium is vulnerable to AF.11) Also, increased AEMD duration is also observed in stroke patients, chronic renal disease patients, scleroderma patients, Behcet's disease patients, and polycystic ovary syndrome patients, further adding to the evidence that it can indicate damage and predict AF.5)7)17)18)19)20) Even though PA′ septum and PA′ tricuspid times were significantly increased in surgical early menopausal patients, the PA′ lateral, intra-RA, LA, and inter-atrial EMDs were not significantly altered. Additionally, it was previously reported that an increase in LA dilatation led to an increase in inter-atrial EMD.10) However, in our study, we did not observe any significant alterations in LA diameter in early menopause patients compared to controls. It is possible that this was due to the comparatively short time between operation and the study enrollment and the small sample size.
There are three main mechanical functions of the LA, representing different periods of the cardiac cycle: reservoir, conduit, and pumping. The LA performs its reservoir function during ventricular systole, a transition occurs between early and middle ventricular diastole, and active pumping occurs during late diastole.4) The LA could demonstrate continued adequate cardiac output by balancing its reservoir, conduit, and pumping functions. These functions are affected by many pathological conditions. Pathological LA enlargement initially occurs in response to increased LA volume and helps to maintain the cardiac output. However, continued LA enlargement results in an impaired Frank-Starling relationship and reduced atrial compliance, depot, and pumping function.4)21)22) In our study, although reservoir, conduit, and pumping functions were reduced in surgical early menopause patients, these alterations were not statistically significant.
Increased atrial volume is associated with paroxysmal and persistent AF23) and leads to increased death in the general population. Furthermore, it has been previously demonstrated that in diabetic cases, reduced passive LA emptying volume is associated with higher end-diastolic left ventricular pressures. Moreover, increased active LA emptying volume is associated with increases in LA contractile compensatory features.17)24) In our study, the LA mechanical functions and active and total emptying volumes were increased in surgical early menopause patients. However, these alterations were not statistically significant.
Previous studies have demonstrated that in addition to intra- and inter-atrial EMD, a decreased A′, which is a feature of the LA contractile function, might predict AF.17)25) In our study, the mitral A wave was significantly lower in surgical early menopause patients compared to controls. However, while the septal and lateral mitral annular A waves were also lower in surgical early menopause patients, this observation was not statistically significant.
Study limitations
The primary restriction of this study was its small sample size. Additionally, AF was evaluated and patients were excluded according to each patient's history. However, none of the patients in this study underwent 24-hour Holter monitoring to further exclude patients with potential AF. Similarly, diabetes mellitus was excluded by patient history, symptoms, and clinical findings, not HgA1c level. Accurate measurement of the diameter, area, and volume in this study were dependent on echocardiographic imaging angles and geometric presumptions, and these parameters are also load-dependent. Pulsed-wave tissue Doppler imaging is restricted by the angle dependency of the technique. Moreover, fine atrial walls are difficult to measure. To reduce these deficits, three sequential cardiac periods were assessed and averaged for each measurement. In addition to volumetric measurements, two-dimensional tension, measured by Doppler-based tension or speckle tracking, is often used to assess LA functions. However, no tension measurements were performed in our study. Finally, we could not assess associations between time since surgery and the echocardiography parameters.
Conclusion
We report a statistically significant impairment in atrial electrical delay and electromechanical functions in surgical early menopause patients. Future clinical trials with larger sample sizes that include patients with other forms of early menopause are necessary to confirm the role of surgical menopause in subclinical cardiac alterations and the onset of AF.
 XML Download
XML Download