

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The klotho gene was identified as an aging suppressor gene in mice, the mutation of which causes multiple premature-aging phenotypes and the overexpression of which extended life span [12]. Aging is the primary risk factor for major human pathologies including cancer. Though klotho-deficient (kl/kl) mice manifested multiple aging-like features, cancer has not been identified in kl/kl mice that may be due to short lifespan. Even though it has been suggested that Klotho may have an anti-cancer effect, the link between Klotho and cancer had remained ill-defined until 2007. A homozygous missense mutation in human KLOTHO gene causing severe tumoral calcinosis with severe defects in mineral homeostasis is the first evidence linking Klotho and cancer [3]. Recent studies demonstrated that expression of KLOTHO gene is suppressed by hypermethylation of DNA at the CpG island in the promoter and the first exon in various cancer cells, including cervical, colorectal, gastric and breast cancers [4567] suggesting that Klotho expression may be closely correlated with tumorigenesis. In addition, multiple studies have reported that Klotho suppresses cancer proliferation and metastasis by inhibiting growth factor signaling such as IGF-1 and TGF-β [89].
Clear cell renal cell carcinoma (ccRCC) is the most common type of renal cancer with increasing incidence [10]. Altered expression and/or activity of growth factor receptor are a primary event in ccRCC development [111213]. Augmented IGF-1 receptor (IGF-1R) signaling has been implicated in proliferation and metastasis in diverse cancers including ccRCC [11]. Clinically, IGF-1R expression has been associated with development of highly invasive metastatic ccRCC with adverse prognosis [1213]. Klotho inhibits IGF-1 signaling in mice [2] and suppresses IGF-1-mediated breast cancer progression [8]. Although Klotho is predominantly expressed in distal convoluted and proximal tubules which are a common origin of ccRCC, little is known about the biological role of Klotho acting on IGF-1R signaling involved in renal malignances and its clinical relevance.
Here, we examined the expression levels of Klotho and IGF-1R associated with the clinico-pathological parameters of ccRCC and molecular mechanism of Klotho suppression of ccRCC progression by IGF-1R. The results indicate that Klotho expression is a favorable prognostic factor of ccRCC and Klotho ameliorates tumor progression via inhibiting IGF-1R suggesting that Klotho regulation acting on IGF-1R is an attractive target for therapeutic intervention for ccRCC.
METHODS
Ethics approval and tissue samples
This study has been approved by the Institutional Ethics Committee of Yonsei University Wonju College of Medicine and has followed the principles outlined in the Declaration of Helsinki. After institutional approval, human kidney tissue samples from patients with ccRCC were obtained (YWMR-12-4-048). Pathologic reports and clinical records were reviewed. The tissue samples were collected from patients diagnosed with ccRCC who had undergone surgery at the Yonsei University Wonju Severance Christian Hospital. Collecting formalin-fixed paraffin embedded (FFPE) and fresh tissues for immunohistochemistry (IHC) and immunoblotting were described previously [14].
Cell culture and materials
Cell culture of Caki1 ccRCC cell-line was previously described [14]. Unless otherwise noted, all chemicals and reagents were obtained from Sigma-Aldrich (St Louis, MO, USA). Recombinant human Klotho protein was purchased from R&D Systems (Minneapolis, MN, USA).
Immunohistochemistry and western blot
Procedures and analysis of IHC and immunoblotting of tissue specimens were previously described [14]. Primary antibodies against Klotho (KM2076 and ab69208), IGF-1R and β-actin (Abcam, Cambridge, MA, USA), p-IGF-1R, p-Akt, Akt, p-Erk1/2 and Erk1/2 (Cell Signaling, Beverly, MA, USA) and GAPDH (Santa Cruz Biotechnology, Santa Cruz, CA, USA) were used for immunoblotting and IHC.
Colony formation and wound healing assay
Cells were cultured with IGF-1 and/or Klotho. Culture medium was changed every three days and colonies were visualized with 1% methylene blue. Colony formation and wound-healing assays were performed as described previously [14].
Statistical analysis
Data analysis was performed with the Prism software (version 6, GraphPad Software, San Diego, CA). For statistical comparisons, a two-tailed unpaired Student's t-test, χ2-test and ANOVA were used to compare the categorical and continuous variables. p-values less than 0.05 and 0.01 were considered significant and represented by single- or double-asterisk, respectively. All data were presented as mean±SEM, unless stated otherwise.
RESULTS
Expression levels of Klotho and IGF-1R in ccRCC
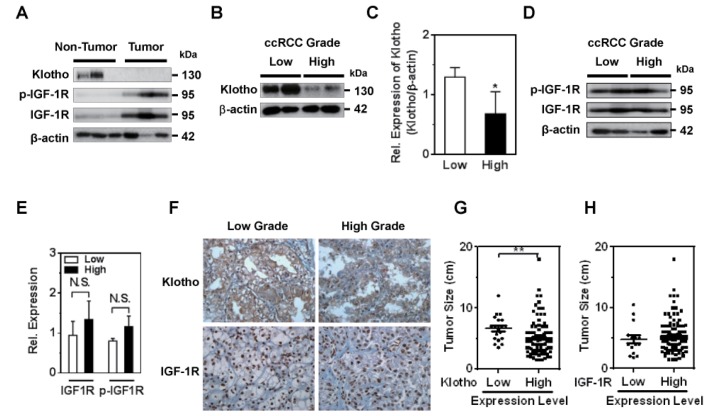
ccRCC is the most common carcinoma originated from the renal tubular epithelium in which Klotho is highly expressed. IGF-1R expression is augmented in diverse human malignancies including ccRCC [1113] and Klotho blunts IGF-1R signaling [2]. Those observations prompt us to examine the correlation of Klotho and IGF-1R expression and clinical significance in ccRCC. To clarify whether expression level of Klotho and IGF-1R is associated with ccRCC development and Klotho inhibition of IGF-1R contributes to tumor progression, ccRCC with pair tissues of carcinoma and adjacent non-neoplastic parenchyma were analyzed using immunoblotting (Fig. 1A). Whereas Klotho expression level was decreased in tumor tissues compared to that of adjacent non-tumor tissues, expression and phosphorylation of IGF-1R were elevated in tumor tissues suggesting that inverse correlation of Klotho and IGF-1R expression may contribute to ccRCC development.
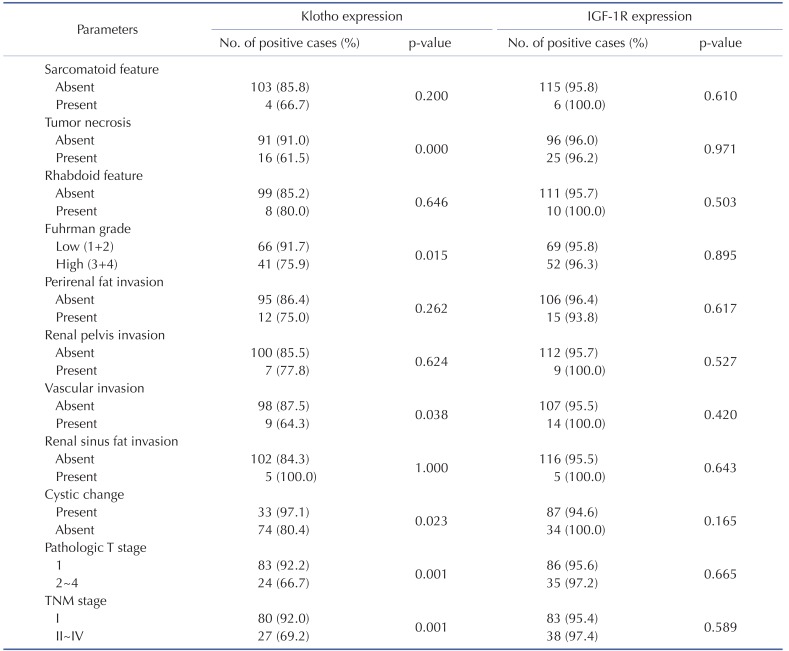
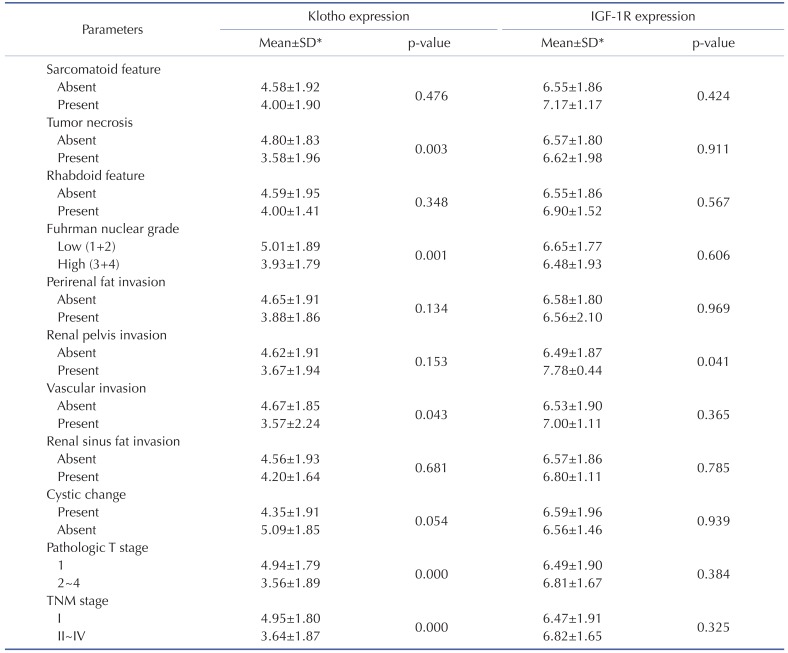
Next, the levels of Klotho and IGF-1R expression in tumor tissue with clinical outcomes were examined using IHC and immunoblotting from FFPE (n=126) and fresh pair samples (n=17), respectively. While the expression level of Klotho expression was clearly low in higher nuclear grade of ccRCC tissues compared to that of lower grade, IGF-1R expression level was not significant between tumor grades (Fig. 1B~E). Consistent with immunoblotting assay, the IHC staining confirmed that Klotho expression was clearly low in higher nuclear grade of ccRCC and IGF-1R expression was not significantly different between tumor grades (Fig. 1F, Table 1 and 2). These results support the notion that the expression level of Klotho was closely correlated with ccRCC progression.
Tumor expression level of Klotho is associated with clinico-pathological parameters of ccRCC
Several clinico-pathological parameters including TNM staging, Fuhrman nuclear grades, and pathologic T stage are used to predict the ccRCC prognosis [15]. TNM staging is the most reliable prognostic factor and Fuhrman nuclear grade is an independent prognostic factor based on nuclear and nucleoli morphology. To determine if Klotho and IGF-1R have any prognostic value, correlation analysis between mean staining score of Klotho and IGF-1R and clinico-pathological parameters was examined. The level of Klotho expression in tumor tissues was significantly lower in the higher TNM stages, Fuhrman nuclear grades, and pathologic T stage (Table 1 and 2). Additionally, Klotho level was significantly higher in the groups of existing tumor necrosis, vascular invasion and absent cystic changes (Table 1 and 2) suggesting that Klotho is the favorable prognostic factor of ccRCC. On the other hand, the expression level of IGF-1R was not statistically significant with clinico-pathological parameters among patients with ccRCC. More importantly, the expression level of Klotho, not IGF-1R, in tumor tissues was significantly correlated with tumor size (Fig. 1G and H). These results suggest that Klotho is more favorable prognostic factor of ccRCC.
Klotho suppresses IGF-1-stimulated ccRCC cell proliferation and migration
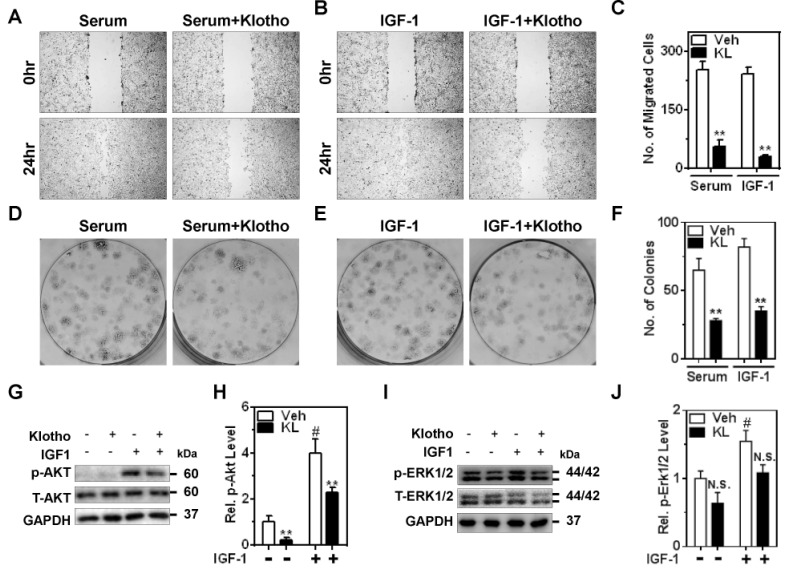
Augmented expression and/or activity of growth factor receptors are primary feature of cancer. Exaggerated IGF-1R signaling has been implicated in invasive metastasis and proliferation of ccRCC [1116]. Next, whether Klotho inhibits ccRCC progression stimulated by serum growth factors including IGF-1 was examined using ccRCC cell line, Caki1. Serum- and IGF-1-stimulated ccRCC cell migration was analyzed via wound-healing assay in the presence of mitomycin C to exclude the effect of cell proliferation. Consistent with previous reports, serum and IGF-1 stimulated migration of Caki1, ability of which was blunted by incubation of purified Klotho protein (Fig. 2A~C). Additionally, serum and IGF-1 facilitated proliferation of Caki1 and Klotho prevented colony formation induced by serum and IGF-1 (Fig. 2D~F). These data suggest that Klotho ameliorates cell motility and proliferation stimulated by serum growth factors such as IGF-1.
Klotho downregulates IGF-1R signaling
IGF-1R governs diverse signaling cascades including a phosphoinositie-3-kinase (PI3K)/Akt and Erk1/2 pathways. Next, the effect of Klotho on IGF-1R signaling in ccRCC was examined. Major downstream effector of IGF-1R is a PI3K/Akt pathway, which is highly activated and genetically mutated in ccRCC [1617]. While IGF-1 activated Akt in Caki1 cells, Klotho blunted basal and IGF-1-stimulated Akt activation (Fig. 2G and H). Although IGF-1 activated Erk1/2 in Caki1 cells, only minor effects were noted on Klotho inhibition of Erk1/2 activation by IGF-1R (Fig. 2I and J). These results suggest that Klotho might have a suppressive role for ccRCC through inhibiting PI3K/Akt-dependent pathway of IGF-1R.
DISCUSSION
Previous studies have shown that Klotho exhibits tumor suppressive function in various cancers [345678918] except hepato cellular carcinoma [19]. Klotho is predominantly expressed in the kidney tubular epithelium which is the origin of ccRCC. Augmented expression and/or activity of growth factor receptor have aggravated ccRCC progression [16]. Altered IGF-1R expression is a hallmark of most cancer including ccRCC, the expression and activity of which have been augmented [518]. The role of Klotho acting on IGF-1R regulating ccRCC progression and its clinico-pathological relevance has been ill-defined. Here, we ask the question whether Klotho exerts tumor suppressive role for ccRCC through inhibiting IGF-1R signaling and its clinical significance. Our data shows the following key findings. First, in tumor tissues, the level of Klotho and IGF-1R expression are low or high, respectively, compared to that of adjacent non-neoplastic parenchyma. Second, the level of Klotho expression is clearly low in higher grade of ccRCC and is closely associated with clinical outcomes in tumor progression. Third, Klotho suppresses IGF-1-stimulated cell proliferation and migration by inhibiting PI3K/Akt pathway. These results provide compelling evidence supporting the notion that Klotho acting on IGF-1R signaling functions as tumor suppressor in ccRCC.
Several observations argue that low expression of Klotho in tumor tissue is associated with a poor prognosis [81819]. Although Klotho is known as a favorable prognostic factor in breast and renal cancers [818], oncogenic function of Klotho facilitating tumor migration and invasion is also suggested in hepatocellular carcinoma [19]. While pathologic poor prognostic factors in ccRCC include the presence of tumor necrosis and vascular invasion [20], cystic change is a favorable prognostic factor in predicting survival of RCC [21]. Our results support previous reports that Klotho is a favorable prognostic factor of ccRCC and extend that Klotho has an additional clinical outcomes such as a presence of cystic change and an absence of tumor necrosis and vascular invasion. Additionally, Klotho expression was decreased in tumor tissues compared to that of adjacent normal tissues suggesting that Klotho expression is closely related to ccRCC development.
IGF-1R signaling has been augmented in ccRCC with poor prognosis [11]. Consistently, IGF-1R expression was much higher in tumor tissues compared to that of adjacent normal parenchyma supporting that overexpression of IGF-1R is related with tumorigenesis of ccRCC. However, IGF-1R expression was weakly associated with clinico-patholgical paramenters of ccRCC in the present study. It is conceivable that IGF-1R expression may be saturable in tumor tissues of ccRCC. These data suggest that Klotho expression is more important prognostic factor for ccRCC than IGF-1R expression.
Altered expression and/or activity of IGF-1R are critical for ccRCC development and progression. Augmented expression of IGF-1R is a typical feature of most types of cancer including ccRCC [1122]. Genetic alterations invlove in initiation and progression of ccRCC. The IGF-1R gene has been transcriptionally downregulated by variety of tumor suppressors including von-Hippel Lindau (VHL) gene, somatic mutation of which occurs in most case of ccRCC [111722]. E3 ligase VHL protein functions as tumor suppressor via inhibiting hypoxia-inducible factor-1α (HIF-1α) whose regulation by VHL is crucial for ccRCC tumorigenesis. Additonally, components of PI3K/Akt pathway, major downstream of IGF-1R, have been frequently mutated in ccRCC [17]. Multiple studies demonstrated that crosstalk between the VHL/HIF-1 and PI3K/Akt pathways is critical for ccRCC progression supporting that altered activity of IGF-1R may contribute to ccRCC tumorigenesis. In addtion, Erk1/2 is downstream target of IGF-1R that regulates cell growth and prolifeartion, activation of which promotes tumor progressoin including RCC [23]. Klotho potentiates activation of Erk1/2 by FGF23 [24] but inhibits its activation by IGF-1R [8]. Although activation of Erk1/2 has been implicated in RCC progression [23], only minor effect of Klotho on Erk1/2 activation were noted in ccRCC suggesting that PI3K/Akt pathway may be major target of IGF-1R involving ccRCC.
Indeed, exaggerated IGF-1R signaling has been aggravated ccRCC progression notoriously resistant to chemo- and radiotherapies [1117]. Genetic or pharmacological targeting IGF-1R signaling inhibition may provide new insights to overcome resistance of conventional chemo- and/or radiotherapy in ccRCC. Thus, Klotho inhibition targeting IGF-1R signaling in ccRCC offers clues for treatment stragegies of ccRCC.
 XML Download
XML Download