

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sarcomatoid carcinoma is an uncommon tumor in the gastrointestinal tract [1]. These tumors have been reported in diverse sites including gallbladder [2], stomach [3], esophagus [4] and colon [5], but are only rarely reported in the small intestine [1,6,7]. Outcome is poor in patients with sarcomatoid carcinoma, because patients usually present with large tumor at extended stages [1]. We report a case of a 62-year-old man with sarcomatoid carcinoma involving the small intestine and review the relevant literature.
CASE REPORT
A 62-year-old man was admitted to Konyang University Hospital due to abdominal pain experienced for one month. His personal and family histories were unremarkable. Physical examination revealed generalized abdominal tenderness. Laboratory tests revealed anemia (hemoglobin, 5.9 g/dL; hematocrit, 18.7%) and neutrophilia (13.0 × 103/µL). Liver and renal function tests were unremarkable.
Examination by esophagogastroduodenoscopy and colonoscopy showed no abnormal findings. Abdominal computed tomography (CT) scan showed wall thickening of the small intestine. A small bowel series showed complete segmental fold effacement of the ileum (Fig. 1). No distant metastasis was detected after the patient underwent a positron emission tomography (PET)-CT scan.
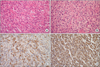
Segmental resection revealed a mass located at the ileum, 40 cm from the ileocecal junction. The resected specimen showed an ulcerofungating mass that measured 15 × 9 × 2 cm in dimension. The cut surface revealed a grayish white, solid, and firm mass, with areas of hemorrhage and necrosis. The mass extended through the entire thickness of the wall of the small intestine, with invasion into the mesenteric fat. The gross and microscopic margins were widely free of involvement. Microscopically, the tumor consisted of spindle and polygonal giant cells. Spindle cells were arranged haphazardly in a fascicular growth pattern, with nuclear hyperchromasia and distinct nucleoli. Discohesive polygonal giant cells have dense eosinophilic cytoplasm and pleomorphic nuclei. The numbers of mitotic figures averaged 15 per 10 high power fields. Lymphatic invasion was present, but the surrounding lymph nodes were free of tumors. No carcinomatous component was recognized. Immunohistochemistry revealed diffuse, strong positive staining for cytokeratin and vimentin. Epithelial membrane antigen and CD68 were focal positive. Smooth muscle actin, S-100, CD34, HMB-45, Desmin and C-kit were negative (Fig. 2). The final diagnosis was sarcomatoid carcinoma of the small intestine.
The patient received 2 cycles of chemotherapy including doxorubicin and dacarbazine. Three months later, PET-CT showed a recurrent mass in the pelvic cavity. After resection of recurrent small bowel mass, the patient restarted chemotherapy with doxorubicin, dacarbazine, ifosfamide and mensa.
DISCUSSION
Sarcomatoid carcinoma is a controversial and rare tumor that displays both carcinomatous and sarcomatous features. It has variety of names including carcinosarcoma, metaplastic carcinoma, spindle cell carcinoma, and pleomorphic carcinoma [1]. For the small intestine, sarcomatoid carcinoma was first described by Dikman and Toker [8] in 1973. Less than 30 cases of small intestinal sarcomatoid carcinoma have been reported in the English language literature to date [1,6,7]. In Korea, only one case of small intestinal sarcomatoid carcinoma has been reported in the duodenum [9].
Clinically, sarcomatoid carcinoma in the small intestine seems to be a disease that affects elderly patients, presenting at a mean age of 57 years [1]. Presenting symptoms include: abdominal pain, intestinal obstruction, palpable abdominal mass, gastrointestinal bleeding, and anemia [6,7,10]. In the present case, the patient had abdominal pain and anemia.
Histologically, sarcomatoid carcinoma may appear with a biphasic or monophasic pattern [1]. A mixture of epithelial-looking and mesenchymal-like cells characterized the typical biphasic pattern. Monophasic tumors show a predominance of the mesenchymal-like component, with minimal to absent epithelioid areas [1]. The presenting case was predominantly composed of spindle cells, with some polygonal cells. No conventional carcinomatous component was present. Monophagic sarcomatoid carcinoma may be confused with other sarcomas due to the absence of carcinomatous features. A wide panel of immunohistochemical markers was performed to sort out a diagnosis from a wide range of differentials, including leiomyosarcoma, epithelioid angiosarcoma, epithelioid malignant peripheral nerve sheath tumor (MPNST), gastrointestinal stromal tumor (GIST), and melanoma. The absence of S-100 and HMB-45 ruled out the possibilities of an epithelioid MPNST and melanoma. A leiomyosarcoma was ruled out in view of smooth muscle actin and desmin negativity. Lack of C-kit and CD34 ruled out the possibility of a GIST and an epithelioid angiosarcoma. Most of the pleomorphic spindle cells expressed both cytokeratin and vimentin. This tumor was suggested to be epithelial in origin and had transformed to a sarcomatous tumor.
The first choice of therapy for a solid tumor is always surgical resection. Surgery is an effective treatment for sarcomatoid carcinoma of the small intestine [1,7]. Neither radiotherapy nor chemotherapy contributes to the survival rate [1]. However, due to the high malignancy of sarcomatoid carcinoma, many patients are diagnosed with the tumor at a late stage and die due to metastasis [1,7,11]. The duration of survival is generally only a few months [1,7]. In this case, although the patient was treated with adjuvant chemotherapy, the tumor recurred within three months after surgery. Informing the patient of the aggressive biological behavior of the tumor and careful follow-up would be necessary for patients.
In summary, we present a case of sarcomatoid carcinoma in the small intestine. As small intestinal sarcomatoid carcinoma demonstrates highly aggressive behavior, radical surgery and short-term follow up are recommended.

 XML Download
XML Download