

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Fournier gangrene (FG), first described by Jean Alfred Fournier in 1883 [1], is an acute and potentially lethal necrotizing fasciitis that involves the skin and soft tissues of the scrotum, perineum and even lower abdominal wall. The common risk factors of this disease include old age, diabetes, alcoholism, malignancy, and an immunocompromised state [2]. The common routes of bacterial entry in FG include urinary tract infection, perianal infection or local trauma to the scrotum and perineum. Early diagnosis, effective debridement and appropriate medical treatment increase the likelihood of survival. Starting with the initial presentation, comprehensive planning of general care to final wound closure is imperative. Although healing by secondary intention, delayed repair, and skin grafting is occasionally appropriate, flap reconstruction is critical, especially when large dead space and vital structures are exposed. Options for regional flaps include pudendal, thigh, gluteal and abdominal flaps. Free tissue transfer is an option available for massive defects. Instead of frequent dressing changes, negative pressure wound therapy (NPWT) is preferable for large wounds until definitive wound closure.
Identification of prognostic factors is essential to establish the optimal treatment plan and to improve the outcome. Poor prognostic factors, such as advanced age, comorbidities, delayed diagnosis and treatment, extension of gangrene, reoperations and laboratory data at diagnosis have been investigated previously.
We conducted an 8-year review of our institutional experience with FG management. The specific aims of our study were to characterize the demographics of FG at our tertiary care center and to analyze different factors affecting patient outcomes and mortality.
METHODS
Study population
After excluding 2 patients from the cohort due to incomplete medical record, we conducted a retrospective study of 41 patients diagnosed with FG and undergoing surgical or medical treatment at our institution during the 8-year period between August 2009 and April 2017. This study was approved by the Institutional Review Board (approval number: AJIRB-MEDMDB-17-460) with approval of a waiver of informed consent. The diagnosis of FG was based on the patient's medical history and physical examination. Patients without complete medical records or photographic documentation were excluded.
Management
Upon admission, each patient was initially treated with empiric broad-spectrum parenteral antibiotics, especially third-generation cephalosporins including aminoglycosides and metronidazole. Initial surgical debridement was performed within the first 12 hours after admission. Microbial cultures obtained in the operating room during each debridement sequence determined subsequent antibiotic management. Between surgical procedures, wound was managed by changing wet-to-dry gauze every 8–12 hours daily or more often as deemed necessary in the ward. For larger wounds, a negative-pressure dressing (CuraVAC, CGBio Inc., Seongnam, Korea) was applied after surgical debridement. Wounds were serially debrided until healthy and viable tissue was visible under local or general anesthesia. Definitive wound management involved healing by secondary intention, through secondary closures, skin grafting, or flap reconstruction. Indications for flap transfer were cavitary deep tissue defects, wounds with wide dead space, and exposed testicles. Regional flap transfers involved perforator flaps. Free flap transfers included anterolateral thigh fasciocutaneous flaps. The advantage of perforator flaps and fasciocutaneous flaps is reduced donor site morbidity in terms of function, pain and contour deformity since the underlying muscle was not included in the flap.
Fecal or urinary diversions were performed in select cases. Patients diagnosed with severe sepsis and patients requiring vasopressors or mechanical ventilation support were treated in the intensive care unit (ICU). Malnourished patients received nutritional support.
Study variables and outcome measurement
We collected clinical and demographic variables. For instance, we ascertained age, sex, etiology, risk factors, and duration of symptoms before admission. Results of physical examination included extent of affected area, laboratory findings, interval between the onset of symptoms and hospital admission, Fournier Gangrene Severity Index (FGSI) and laboratory risk indicator for necrotizing soft tissue infection (LRINEC) scores [34]. We also determined the presence of systemic inflammatory response syndrome (SIRS) on admission, comorbidities, number of subsequent debridements, methods of wound reconstruction, requirement for intestinal and urinary diversion, length of stay in the ICU and total hospital stay, and mortality. Patients were considered to have chronic kidney disease (CKD) if they had 2 previous measurements at least 6 months apart of serum or plasma creatinine of at least 150 µmol/L (1.7 mg/dL) in men or 130 µmol/L (1.5 mg/dL) in women, whether or not they underwent dialysis. Mortality was defined as disease-related death during the hospital stay. The presence of SIRS at admission was defined by the presence of 2 or more of the following features: a temperature of >38℃ or <37℃, a heart rate >90 beats per minute, a respiratory rate > 20 breaths per minute, a white blood cell count >12,000 or <4,000 cells/mm3 or 10% immature bands.
The extent of gangrene was divided into 2 grades to assess the degree of spread: limited grade was defined as necrotizing fasciitis localized in the “Y” area of the perineum, scrotum and penis, vulva, perianal or inguinal region (Fig. 1) while extended grade referred to extension of the disease to all other areas.
We also used clinically validated scoring systems, such as the LRINEC and FGSI calculated using patient admission data, to assess the severity of infection (Fig. 2). FGSI was obtained by combining clinical (temperature, heart, and respiratory rates) and laboratory parameters (hematocrit and leukocyte count, serum sodium, potassium, creatinine, and bicarbonate) at admission. In this index, each parameter was assigned 0 to 4 points, and FGSI was calculated by adding the points of each parameter.
Treatment outcomes included mortality, length of ICU stay and total hospital stay, number of repeat debridements, and methods of reconstruction. Mortality was defined as disease-related death during the hospital stay and the duration of ICU and hospital stay was measured in days.
Statistical analysis
An independent biostatistician conducted the analysis to assess whether clinical variables were significant predictors of treatment outcomes in this retrospective observational sample. Descriptive statistics and baseline comparisons of the 2 subsamples of survivors and nonsurvivors were addressed. Chi-square or Fisher exact tests were used for categorical variables, while t-tests or Wilcoxon rank-sum test were employed for continuous variables. To examine the association between clinical variables and the treatment outcomes, multivariate logistic and linear regressions were also conducted with stepwise selection technique. The values for the numbers of cases, persons, days, years, and months were expressed as original amounts and percentages to one decimal place. Odds ratios (ORs), 95 % confidence intervals (CIs), and corresponding P-values were calculated for each model. A P < 0.05 was considered significant. The curve fitting was performed with R language, Version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
The 41 patients included 33 males (80.5%) and 8 females (19.5%), with a mean age of 54.4 years (range, 24–79 years). Diabetes mellitus coexisted in 19 patients (46.3%) and hypertension in 15 (36.6%). Seventeen patients (41.5%) were current smokers. Seven patients (17.1%) had premorbid CKD. Three patients (7.3%) presented with malignant neoplasm. The mean duration from the symptom onset to hospital admission was 9.1 days (range, 1–45 days). Demographic characteristics and the proportion of patients with a medical history or comorbidities are described in Table 1. Demographic characteristics of the survival and nonsurvival group were similar at baseline, except for the presence of CKD. Baseline clinical data including vital signs and laboratory values were also not significantly different between the two groups (Table 2). In terms of FG severity, the mean FGSI and LRINEC scores were 6.3 (range, 0–16) and 7.5 (range, 0–12) for the overall group, 5.7 (range, 0–14) and 7.4 (range, 0–12) for survivors, and 8.2 (range, 2–16) and 7.9 (range, 4–12) for nonsurvivors, without significant difference. In terms of baseline nutritional status, mean albumin scores were not significantly different.
Wound characteristics of gangrenes and their management are summarized in Table 3. Etiology or origin was clear in 32 cases (78.1%): the most frequent was urogenital lesions (17 cases, 41.5%). Notably, there were 23 patients of gangrene with limited grade and 18 patients with extended grade, which varied significantly between survivors and nonsurvivors (P = 0.028). No other factors varied significantly.
Prevention of fecal contamination was attempted by diverting-colostomy in 11 patients (26.8%), and 1 patient (2.4%) required cystostomy for urinary diversion. Orchiectomy was required in 4 patients (9.8%).
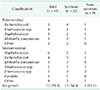
Microbiological cultures were obtained in all cases. A single microorganism was isolated in 22 patients (53.7%), and multiple microorganisms were found in 7 patients (17.1%). No identifiable microorganism was cultured in 12 cases (29.3%). The most frequent bacterial agent cultured from the deep infected tissue was Escherichia coli (31.0%). Table 4 summarized the wound culture results.
In this study, 9 patients died from disease-related events, yielding a mortality rate of 22.0%. Septic shock was the cause of death in all nonsurvivors. Other concurrent complications were variable organ dysfunction, septic embolism, and gastrointestinal bleeding due to disseminated intravascular coagulation. No patient died due to unexpected complications after surgical procedures. The average follow-up was 44 months. Twenty-one patients (65.6%) in the survival group and all patients in the nonsurvival group were treated in the ICU for at least one day, due to unstable vital signs, and required vasopressors or mechanical ventilation support. The overall length of hospital stay ranged from 1 to 166 days with a mean of 47 days. The mean length of hospital stay for nonsurvivors was 29 days (range, 1–73 days). Both survivors and nonsurvivors showed similar outcomes with regard to the length of ICU and total hospital stay and need for multiple surgical debridements (Table 5). Five survivors needed flap reconstruction, including 3 free flaps (Fig. 3). The wounds of 8 patients were covered with split-thickness skin grafts. Ten cases of wounds were repaired secondarily after controlling the infection. The wounds in the remainder of cases were healed without surgical intervention.
The following factors were associated with increased mortality rates in univariate model; extended grade (P = 0.032) and CKD (P = 0.024). Limited-grade gangrene was used as the point of reference to calculate the power of the extent of the gangrene in the logistic regression model. These 2 factors were also significant in multivariate models with stepwise technique (P = 0.035 and P = 0.021, respectively, Table 6). According to multivariate logistic regression analysis, premorbid CKD was a significant predictor of flap reconstruction (OR, 17.3; 95% CI, 1.3–451.0; P = 0.037).
Factors predicting the length of ICU stay over 7 days in univariate analysis were etiologies other than urogenital origin (OR, 9.6; 95% CI, 1.6–86.9; P = 0.022), and extended-grade FG (OR, 16.0; 95% CI, 2.0–193.9; P = 0.014). According to multivariate logistic regression model, extended grade (OR, 21.0; 95% CI, 4.3–162.5; P = 0.001, Table 7) was the main predictor of duration in ICU over 7 days. The extent of the gangrene predicted the overall length of hospital stay in multivariate model (coefficient, 0.9; 95% CI, 0.4–1.4; P = 0.001).
DISCUSSION
Despite the development of various treatment modalities, antibiotic therapy, and intensive care, FG is still a fatal disease with a mortality rate as high as 20%–50% [567].
Among well-known risk factors, diabetes mellitus (DM) is the most reported comorbidity associated with this disease [8910]. The prevalence of DM among FG patients ranges between 50% and 70% [810]. In the present study, 19 out of 41 patients (46.3%) were diagnosed with diabetes. Although substance abuse may play a role in the prognosis due to a higher prevalence of alcohol abuse and smoking in FG patients than in general population [11], we found no relationship between smoking and treatment outcomes. Probably, smoking cessation just before hospital admission might still affected disease progression.
It is a common belief that patients with diabetes are generally more susceptible to infections. Although the existence of diabetes increases the risk of FG, the effect of diabetes on the treatment outcome is disputed. Studies associated diabetes with a more progressive and fatal outcome resulting from decreased phagocytic and intracellular bactericidal activity and neutrophil dysfunction [9]. On the other hand, Laor et al. [3] concluded that although diabetes contributes to FG, it did not affect the results of treatment. Renal insufficiency occurred in 7 out of 30 patients, and resulted in 6 deaths. Therefore, they reported that renal insufficiency was an important predictor of treatment outcome.
Although FG is associated with decreased immune function in diabetes patients, impaired renal function appears to be the underlying factor influencing the aggravation of FG. Several reports suggested that premorbid renal impairment was a risk factor for mortality [1213]. The difficulty associated with estimating the actual risk of infection in diabetic patients is mainly due to the fact that diabetes is not solely a disturbance of glucose metabolism but instead a chronic inflammatory condition characterized by chronic vascular and renal diseases, with each of these changes altering the response to pathogens. Therefore, it seems near impossible to conclusively answer the question of whether ‘diabetes’ or diabetes together with all its renal complications predisposes to infection. Based on the results of the study, diabetes per se does not have a crucial role in treatment outcomes of Fournier gangrene, whereas diabetic renal complications do affect the outcome probably because well-controlled glycemic level in type 2 diabetic patients has little impact on pathogen susceptibility, whereas continuous hyperglycemia in diabetes increases the susceptibility to infections [14]. Thus, end-stage renal disease without appropriate glucose control represents the real cause of unsatisfactory treatment response. Patients with necrotizing soft tissue infection and decreased renal function warrant more intensive treatment [15]. In this study, CKD increased the mortality and increased inflammation, poor control of infection, and thus severe tissue destruction indicate the need for flap reconstruction in CKD patients.
In CKD patients, SIRS might exacerbate pre-existing renal dysfunction. In these sense, creatinine level probably is an important biomarker for the prognosis of the disease. As many patients diagnosed with necrotizing fasciitis experienced acute pre-renal type renal failure at initial presentation and increased levels of serum creatinine during disease progression, the initial laboratory value and scores reflecting kidney function and systemic inflammation were analyzed statistically. The results suggest that serum creatinine and blood urea nitrogen were not associated with the prognosis since the patients were mostly severe with late stage disease. However, serial serum creatinine levels are appropriate biomarkers of disease progression, and a further study will establish the results.
The control of wound infection is important in patient care. All the wounds of the survivors were eventually covered either with secondary intention or with reconstructive procedures before discharge from hospital, suggesting that wound management was successful. In our study, 20 patients were treated with NPWT. As a treatment protocol, NPWT was applied on a large raw surface wound (approximately the size of fist) to reduce the frequency of dressing changes. Otherwise, smaller wounds were managed with frequent dressing changes using conventional soaking gauze. Univariate regression analysis revealed that NPWT was associated with longer ICU stay (P = 0.002), multiple surgical debridements (P = 0.013), and longer hospital stay (P = 0.017). However, multivariate analysis showed no correlation after controlling the covariates. These results suggest that larger wounds might prolong the treatment process and not NPWT per se.
Palmer et al. [16] reported that the area of FG affected the treatment outcome. Benizri et al. [17] also found that local involvement was associated with reduced mortality, when compared with extensive body involvement. For technical reasons, it is not feasible to measure the surface area of disease involvement, especially in the perineal area. Instead, we categorized the extent of gangrene into 2 groups, which were localized to the perineal, perianal, and inguinal region or beyond. We also found a relationship between the area of necrosis and prognosis: mortality rate was significantly higher when the gangrene extended beyond the perineal and inguinal area. Similar results were reported in previous studies, in which the extent of disease was categorized into 3 grades [18].
The organisms isolated in FG are the same bacteria that constitute the normal skin and mucosal flora of urogenital and perianal region. These colonizations are frequently polymicrobial and probably involve both aerobic and anaerobic organisms [19]. Infections with E. coli, and Klebsiella, Staphylococcus, Streptococcus, Proteus, Pseudomonas, Bacteroides, and Clostridium spp. are common [20]. As reported previously, E. coli was the most common, and occurred in 9 of our cases. Although we isolated few anaerobes, their presence was strongly suspected based on crepitus and subcutaneous emphysema.
Despite its meaningful findings, the retrospective nature of our study is associated with inherent limitations. We focused on mortality and perioperative outcomes within our cohort, due to poor patient retention for long-term follow-up. In addition, general care techniques and wound management strategies have evolved significantly over the period covered by our patient registry, which may also have impacted on our results. These factors play a critical role in any evaluation of our work.
In conclusion, Fournier gangrene with extensive soft tissue necrosis and pre-existing CKD is associated with poor prognosis and complicated patient management. Prompt recognition of dissemination and premorbid renal function is essential to reduce mortality and establish a management plan for this disease.









 XML Download
XML Download