

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The process of deceased donor recovery and procurement in Asia is not as well structured as are those systems in Europe and America [1]. Confucianism-based thinking in East Asia has led to some hesitance to donate one's organs, given the belief that one's body is a gift from one's parents that should not be damaged [2]. The mean wait time for a deceased donor kidney transplant (KT) in South Korea is 1934 days [3]. In order to expand the kidney donor pool, the use of organs has been extended to include expanded criteria donors (ECDs) and donors after circulatory death (DCD). Receiving a KT from an ECD or DCD is considered more beneficial than is remaining on the waiting list and continuing dialysis [45].
The perception that acute kidney injury (AKI) disqualifies a potential donor kidney has led to loss of many viable organs [6]. However, a donor kidney with AKI from a toxic or ischemic insult can fully recover its renal function [7]. Therefore, the use of deceased donor kidneys with AKI has been considered an alternate plan to using a healthy organ. Prior studies have shown that the outcomes in recipients of kidneys with AKI are comparable [89]. Several standardized classification systems for AKI status have been developed in clinical practice [10]. The Acute Kidney Injury Network (AKIN) criteria for the diagnosis of AKI in deceased donor transplantation are useful to predict the development of delayed graft function (DGF) in KT [11].
In this study, we investigated the clinical outcomes of KT from deceased donors with terminal AKI, which was defined using the AKIN criteria and ECD classification.
METHODS
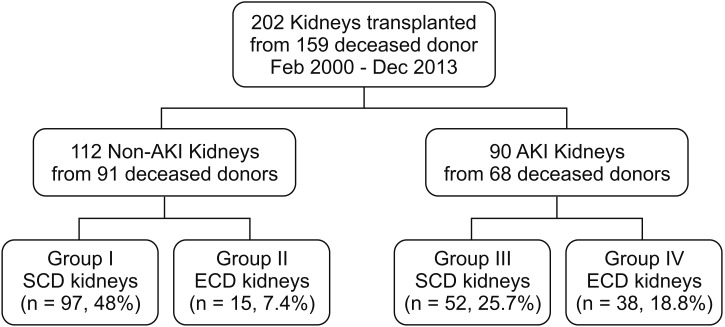
In this retrospective study, we reviewed the medical records and electronic transplant registry of KT recipients at Seoul St. Mary's Hospital, The Catholic University of Korea, between February 2000 and December 2013. This study was conducted according to the Declaration of Helsinki and approved by the Institutional Review Board of The Catholic University of Korea (No. KC17RESI0397). We analyzed 202 deceased donor KTs from 159 brain dead donors. The data included information regarding 53 ECD grafts and 90 grafts with AKI. Based on the ECD classification and AKIN criteria, the recipients were divided into 4 groups. In group I, 97 recipients received non-AKI and SCD kidneys. Fifteen recipients received ECD kidneys without AKI in group II. In group III, 52 recipients received kidneys with AKI and SCD, and 38 recipients received ECD kidneys with AKI in group IV (Fig. 1).
Definitions and assessments
All deceased donors older than 60 years, and those 50–59 years of age that met 2 of the following criteria were classified as ECD based on United Network for Organ Sharing definitions: (1) history of hypertension, (2) cerebrovascular accident as a cause of brain death, and (3) final preprocurement serum creatinine (SCr) level >1.5 mg/dL [12].
Deceased donors also were classified according to the AKIN criteria. AKI stage 1 is defined as an absolute increase in the last SCr level by 0.3 mg/dL or higher, a 50% or higher increase in the last SCr level from the level on the day admission, or a reduction in urine output (documented oliguria, <0.5 mL/kg per hour for >6 hours). Stage 2 was defined by an increase in the last SCr of more than 200%–300%, or a reduction in urine output (documented oliguria, <0.5 mL/kg per hour for >12 hours). Stage 3 was defined as an increase in the last SCr of more than 300% or a reduction in urine output (documented oliguria, <0.3 mg/kg per hour for >24 hours or anuria for at least 12 hours) [13]. Deceased donors were compared based on their sex, age at transplantation, body mass index, cause of death, history of hypertension and diabetes mellitus, admission SCr, preretrieval SCr, preretrieval estimated glomerular filtration rate (eGFR), last urine volume, central venous pressure, mean arterial pressure, and days of intensive care unit (ICU) stay. The SCr was measured on the day of admission to our hospital for the pronouncement of brain death. The final SCr level was measured immediately before organ recovery.
The following variables of the recipients were compared: gender and age at transplantation; cause of end-stage renal disease; type and duration of renal replacement therapy; number of transplantations; number of human leukocyte antigen mismatches and other immunologic factors; nephron mass index (donor kidney weight to recipient body weight ratio [Kw/Rw]; g/kg); number of renal arteries; total ischemic time; modification of diet in renal disease (MDRD) glomerular filtration rate (GFR) on posttransplant days 2, 7, and 1 month, 3months, 6 months, 1 year, 2 years, 3 years and 5 years; incidence of acute rejection (AR) episodes; incidence of DGF episodes; duration of graft function and patient survival. DGF was defined as the need for dialysis in the first week posttransplantation. Renal allograft loss was defined as graft nephrectomy, resumption of ongoing dialysis or return to the pretransplantation SCr level. Patient death with a functioning graft was censored.
Statistical analysis
One-way analysis of variance (ANOVA) for continuous variables and the chi-square test for categorical variables were used to compare data among the 4 groups. Turkey honestly significant difference test was used as post hoc method in ANOVA. All data were expressed as mean standard deviations. The Kaplan-Meier method (log-rank test) was used to compare patient and graft survival rates. Data were censored at the time of death, or at the last available follow-up. Statistical significance was defined as a P-value < 0.05. All statistical analyses were carried out using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA).
RESULTS
Donor characteristics
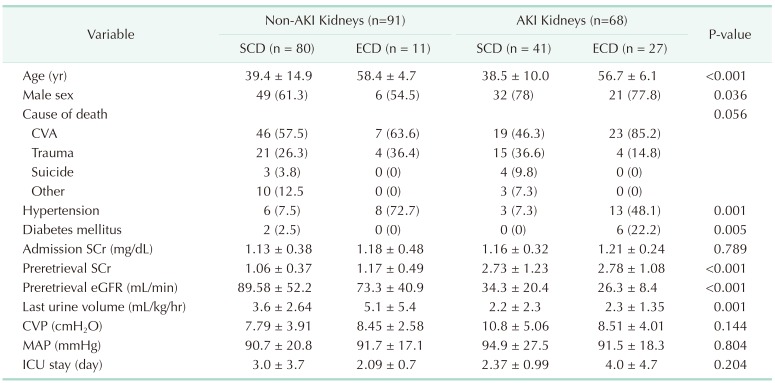
There was insignificant difference in the donor SCr on the admission day across the 4 groups (P = 0.789). However, the preretrieval donor SCr was higher (P < 0.001), while the preretrieval donor eGFR was lower in the AKI groups than they were in the non-AKI groups, respectively (P < 0.001). The last donor urine volume was also smaller in the AKI groups than it was in the non AKI groups (P = 0.001) (Table 1).
Recipient characteristics by group
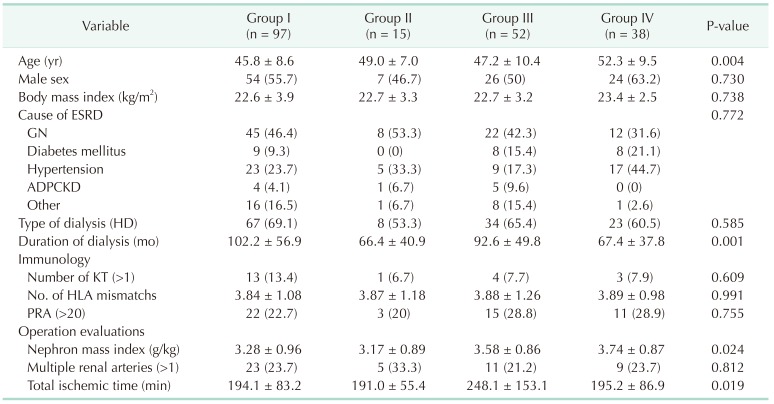
There were significantly different baseline characteristics across the 4 groups. According to the group classification, the median patient age in ECD groups (groups II and IV) was older than that in the non-ECD groups (P = 0.004). The duration of dialysis was significantly shorter in the ECD groups than it was in the non-ECD groups (P = 0.001). The nephron mass index (g/kg) was largest in group IV (P = 0.024). The total ischemic time was longest in group III (Table 2).
Graft renal function, AR episodes, and DGF
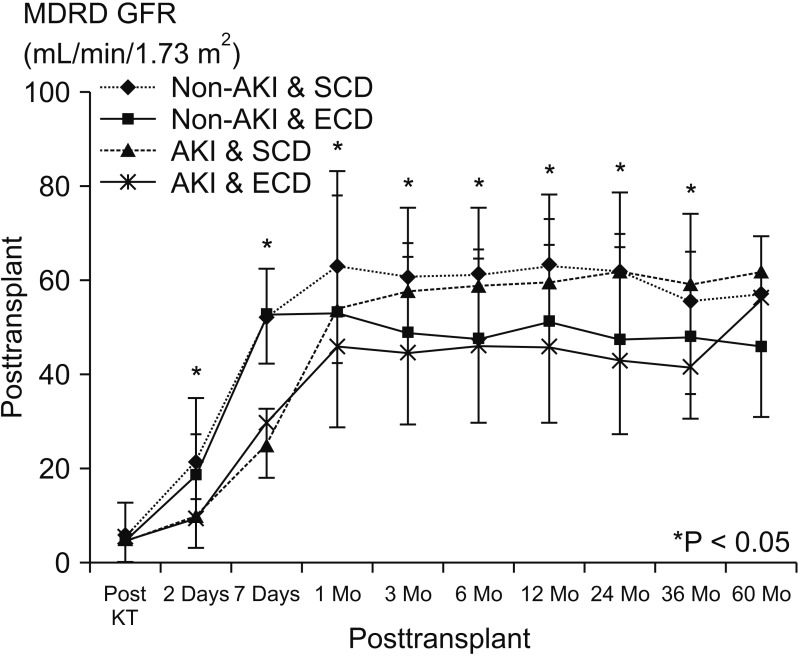
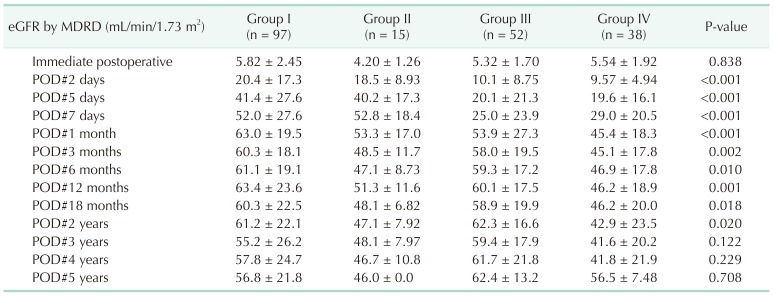
The mean MDRD GFR levels among the 4 groups were significantly different for up to 2 years posttransplantation (P = 0.02). However, 3–5 years after transplantation, the MDRD GFR levels were not significantly different across the groups (P = 0.122, P = 0.229, P = 0.708, respectively) (Table 3, Fig. 2). Although the incidence of DGF was significantly more frequent in patients in the AKI group than it was in those in non-AKI groups (8.13%, 0%, 25.0%, 23.7%, respectively; P = 0.008), the incidence of biopsy-proven AR was comparable among the groups (P = 0.463).
Graft and patient survival
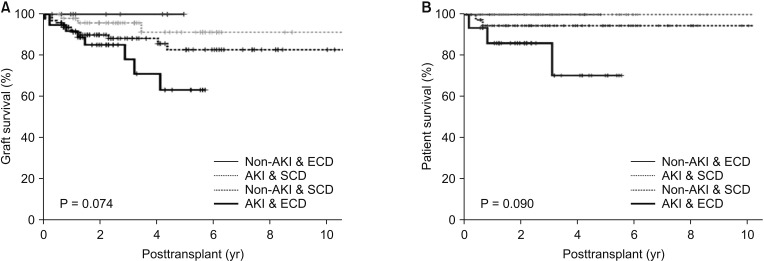
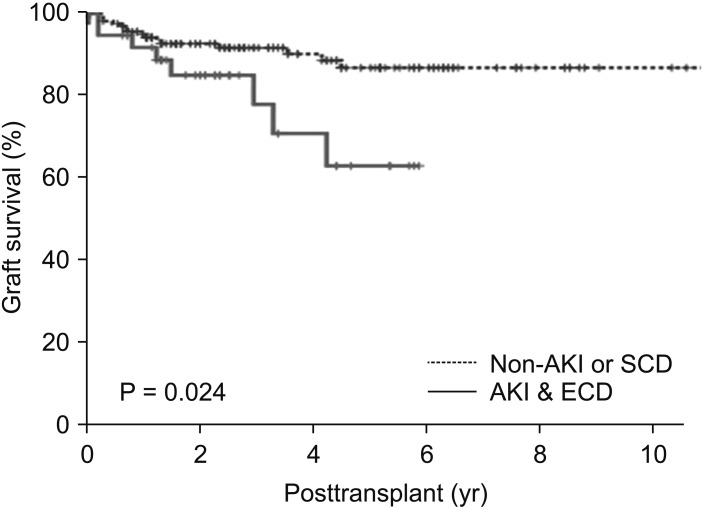
Actual graft and patient survival rates were also similar among the groups, with a mean follow-up period of 40.3 months (P = 0.114, P = 0.094, respectively) (Table 4). Graft survival rates at 1-, 2-, and 5-year posttransplantation were: 91.2%, 89.9%, and 82.7%, respectively, in group I; 100% in group II; 98.0%, 95.8%, and 91.2%, respectively, in group III; and 91.8%, 85.0% and 63.0%, respectively, in group IV. Patient survival rates at 1-, 2-, and 5-year posttransplantation were: 97.8%, in group I; 100% in groups II and III; and 94.4%, 94.4% and 88.1%, respectively, in group IV. There were no significant differences in graft survival rate (P = 0.074) or actual patient survival rate among the 4 groups (P = 0.090) (Fig. 3). However, the long-term allograft survival rate was significantly lower in group IV than it was in the other groups (P = 0.024) (Fig. 4).
DISCUSSION
AKI has diverse causes. AKI can also be relatively benign, with a minimal elevation in SCr levels, or devastating and lead to anuric renal failure [14]. One third of AKI in hospitalized patients represents transient azotemia. However, transient azotemia is also independently correlated with an increased risk of death [15]. AKI frequently develops in patients who become deceased donors, because these patients are critically ill in ICUs and are subject to both ischemic and nephrotoxic insults [16]. DGF manifests as severe ischemic-reperfusion injury (IRI) in the kidney graft [17]. Kidney grafts with preexisting AKI prior to transplantation may be more vulnerable to ischemic injury during recovery, and additional injuries as calcineurin inhibitor toxicity [11].
In transplantation, IRI negatively effects kidney function. There are also several potential etiologies for graft fibrosis, including the immune response and nonimmune factors (e.g., drug toxicities, infections, and urinary tract obstruction) [18]. Hypoperfusion due to shock or rhabdomyolysis after brain death can cause warm ischemia, which may develop prerecovery AKI. Warm ischemic time is associated with irreversible cell damage leading to DGF and primary dysfunction [19]. A preexisting allograft tissue injury may affect the graft's function until natural repair is completed. In nontransplanted kidneys, the phases of AKI consist of initiation, repair, and recovery; this process may continue for up to 6 months [2021]. Due to this potentially prolonged recovery time after AKI, the rates of DGF are greater in donors who have elevated creatinine levels than they are in those without [22]. However, recent studies have shown that there are comparable outcomes after KT from donors with and without AKI [89]. Hall et al. [23] found that the rates of DGF increased as the AKI stage increased; however, there was no significant difference in the 1-year graft survival between AKI and non-AKI groups. Heilman et al. [24] also found that there was no difference in 1-year graft survival or 1-year eGFR between the AKI and control groups. Although the high incidence of DGF did not suggest a poor outcome in AKI donors, DGF itself remains an important risk factor for AR. DGF in non-AKI kidneys developed frequently from AR, which led to poor allograft outcomes [172526].
With regard to baseline characteristics, the duration of dialysis was longest in group I, although the nephron mass index was larger in AKI groups. These findings may reflect that recipients on the waiting list prefer to receive grafts without AKI; in particular, they prefer SCD kidneys without AKI.
We investigated the clinical outcomes of KT from deceased donors with AKI. AKI was defined using the AKIN criteria and ECD classification. The incidence of DGF was higher in the AKI groups than it was in the non-AKI groups. The graft function (MDRD GFR levels) among the 4 groups was significantly different for up to 2 years posttransplantation. After 3 years (and persisting until at least 5 years after KT), the MDRD GFR levels did not differ significantly among the groups. In group IV, the graft function may be affected by both AKI and ECD. It seems that after completion of the repair process, preexisting AKI did not affect the long-term outcome of the allograft kidney [11]. In this study, we found that there was no significant difference in graft survival or patient survival among the 4 groups. According to our past report, ECD may have less of an effect on graft survival and patient survival than previously thought in spite of the incidence of DGF was higher than SCD. There are 2 possible reasons for this result. One is the short cold ischemic time (mean, 4.05 ± 2.18 hours), and the other is the ethnic homogeneity of Koreans [27]. However, the long-term allograft survival rate was significantly lower in group IV compared than it was in the other groups. We can assumed that this subgroup analysis showed a statistically significance because of the negative synergic effect from ECD and AKI groups. Therefore, KT from ECD kidneys with terminal AKI must be carefully considered.
This study has several limitations. First, this was a retrospective study, which makes it vulnerable to bias in general. In addition, the subgroup analysis made up between group IV and the other groups could be prone to the statistical bias of random assignment. Second, according to the Korean guidelines for the management of deceased donors, it is recommended that potential deceased donors be transferred to an appointed institution for solid organ procurement. In this study, the final donor SCr levels were typically measured within 48 hours of the day of admission (and therefore measurement of the baseline SCr level). Therefore, the incidence of AKI may have been underestimated. Lastly, we did not include the AKIN staging categorization in this study. In stage 3, the graft discard rate may have been overestimated. Therefore, the DGF rate and follow up GFR levels could be different according to the stage of AKI.
In conclusion, 42.8% of deceased donors were diagnosed with AKI, while 23.9% were defined as ECD. As the waitlist population for kidneys has increased, using ECD organs with AKI has become a more important alternative. There is no significant difference in graft and patient survival rates with and without AKI. So, the utilization of renal grafts from ECDs with terminal AKI is a feasible approach to address the critical organ shortage.

 XML Download
XML Download