

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The long-term prognosis for patients with breast cancer stage IIIC has been reported to be generally poor compared with those in other stages, with 5-year disease-free and overall survival rates of about 70% and 85%, respectively [123456]. Patients with stage IIIC disease are considered to have pathologic nodal status N3 (pN3; metastases in 10 or more axillary lymph nodes; or in infraclavicular [level III axillary] lymph nodes; or in clinically detected ipsilateral internal mammary lymph nodes in the presence of 1 or more positive level I, II axillary lymph nodes; or in more than 3 axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by sentinel lymph node biopsy but not clinically detected; or in ipsilateral supraclavicular lymph nodes), regardless of tumor size (T stage), according to the 6th and 7th American Joint Committee on Cancer Tumor Node Metastasis (AJCC TNM) staging system [78]. However, the nodal stage of breast cancer, which classifies disease according to the number of metastatic axillary nodes, is further subdivided into prognostic subgroups based on pathologic and molecular characteristics [91011].
The metastatic axillary lymph node ratio (mALNR), defined as the number of positive axillary nodes divided by the number of dissected axillary nodes, is known to be a significant prognostic factor not only in breast cancer, but also in many other types of cancer [12]. Generally, patients with a large number of metastatic lymph nodes have high mALNR and poor prognosis [1314].
Over the recent decades, the prognosis of advanced breast cancer, such as stage IIIC was improved according to development of multimodality treatment (including radical surgery, chemotherapy, radiotherapy, target therapy) [910]. Several studies have suggested the presence of heterogeneous subgroups with different pathologic and bio-molecular characteristics that could influence prognosis within the same stage [9101115]. Thus, patients with certain clinicopathologic features could be expected to have a better prognosis despite a high number of metastatic axillary nodes. Our study was designed to evaluate the prognostic value of mALNR in a group of stage IIIC (pN3) advanced breast cancer patients who received multimodality treatment including mastectomy with axillary dissection, and radiotherapy, endocrine therapy, and target therapy.
METHODS
We analyzed medical records from the breast cancer registry program of the Department of Surgery, Cheil General Hospital and Women's Healthcare Center, Dankook University College of Medicine, Seoul, Korea. Two hundred ninety-seven cases were collected from 3,787 patients who underwent surgery between 1990 and 2010 according to this database. Inclusion criteria were cases with pN3 nodal status (stage IIIC) breast cancer according to AJCC TNM staging system 6th and 7th edition. All patients had undergone mastectomy with more than level II or level III axillary dissection. Cases were excluded if follow-up data were unavailable. The median follow-up period was 60 months (range, 10–302 months). All cases received adjuvant treatment including standard chemotherapy, radiotherapy, endocrine therapy, and target therapy. However, we did not analyze the various types of chemotherapy regimens.
We separately examined the mALNR (number of positive axillary nodes/number of dissected axillary nodes) as a predictor of long-term prognosis. To find a cutoff value of the mALNR, we analyzed the prognoses in patients with a variety of mALNR values. Using univariate analyses for both disease-free and overall survival according to mALNR, the survival difference was most significant when a cutoff value of 0.65 was used. Therefore, patients with a mALNR less than 0.65 were grouped as Low65, and the others were grouped as High65.
All statistical analyses were conducted using SPSS ver. 19,0 (IBM Corp., Armonk, NY, USA). Prognostic parameters considered were age (≤35 years vs. >35 years), menopause status (premenopause or postmenopause), neoadjuvant chemotherapy (not administered vs. administered), operation method (partial vs. total), axillary dissection (level II vs. level III), tumor size (≤2 cm vs. > 2 cm), histologic grade (1 vs. 2 & 3), nuclear grade (1 & 2 vs. 3), estrogen receptor (ER) (−: negative vs. +: positive), progesterone receptor (PR) (− vs. +), Her2 (− vs. +), p53 (− vs. +), and mALNR (Low65 vs. High65). To evaluate correlations between mALNR and clinical-pathologic parameters, data were cross-tabulated (chi-square test/2×2 table; Pearson or Fisher exact test). Univariate analyses with disease-free and overall survival were evaluated using the Kaplan-Meier method, and comparisons between groups were analyzed by the log-rank test. Multivariate analysis was performed on significant prognostic parameters according to univariate analysis using the Cox proportional hazard model in forward stepwise regression to evaluate the independent power of each variable. Statistical significance was set at P-value < 0.05 (95% level of confidence).
RESULTS
Comparison of clinicopathologic features according to mALNR
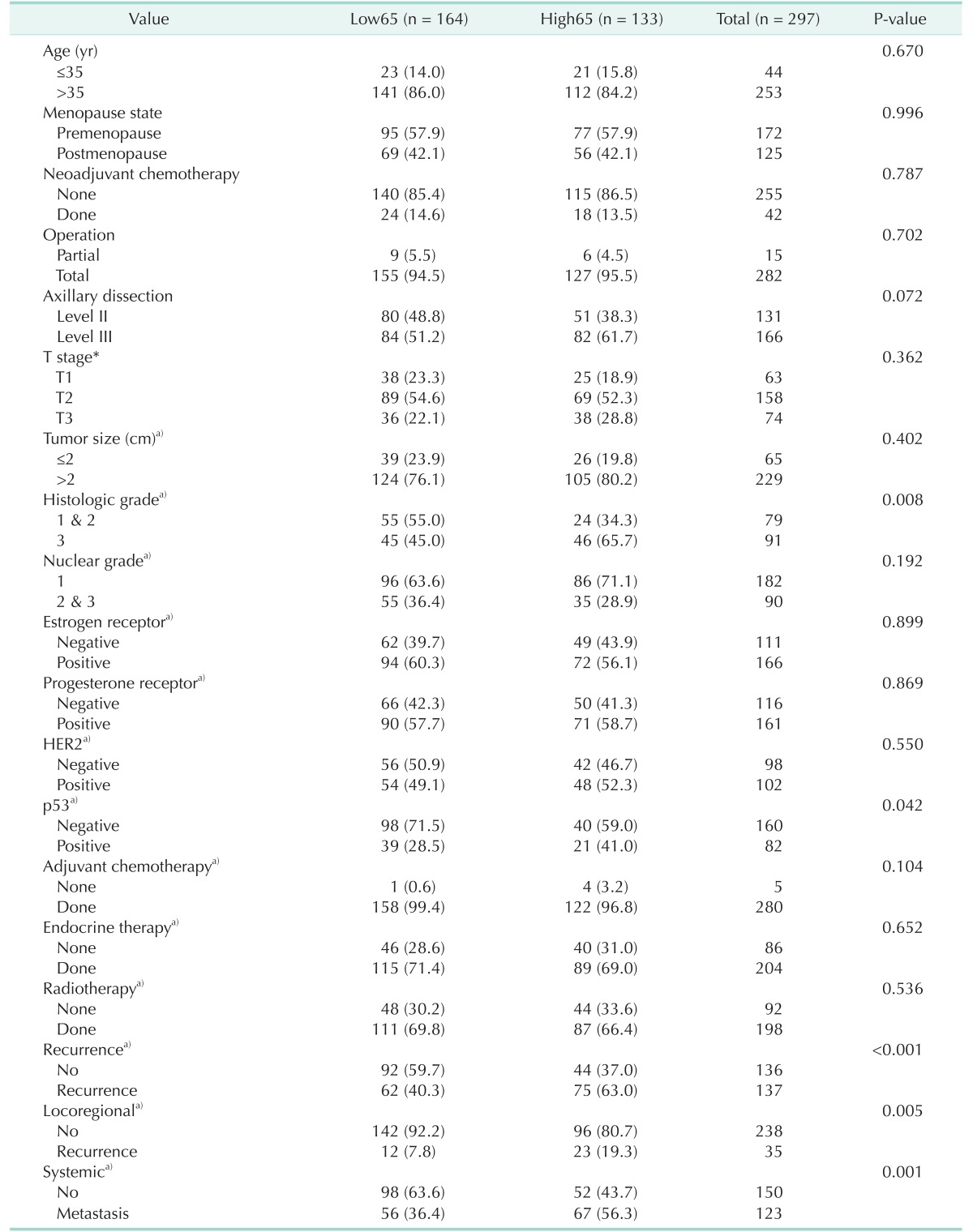
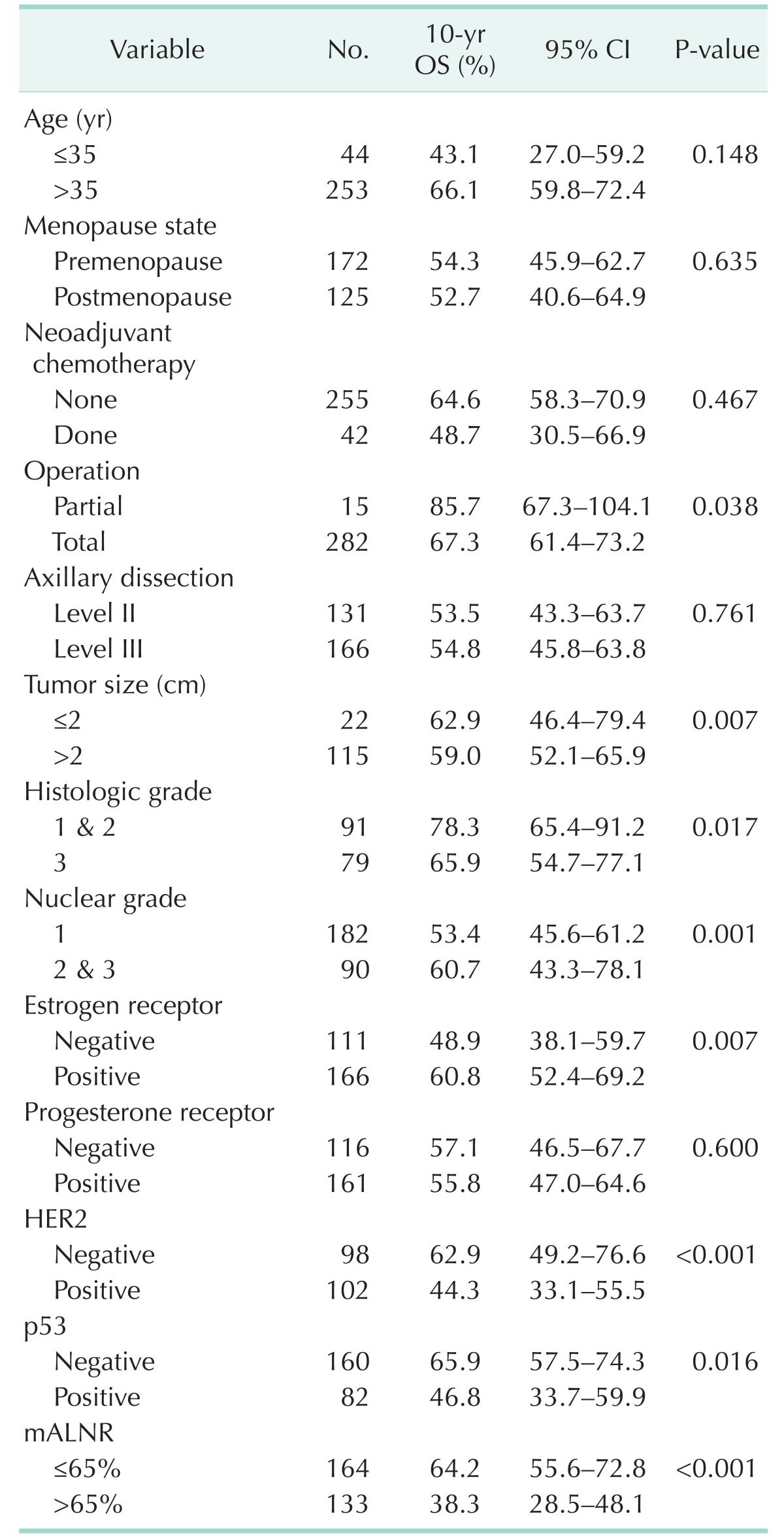
The mean age (±standard deviation; SD) of the 297 patients was 47.3 ± 9.9 years (range, 24–77 years). As shown in Table 1, with the exception of histologic grade (P = 0.008), p53 (P = 0.042), and recurrence (P < 0.001), the clinicopathologic features were well balanced between the two groups of patients.
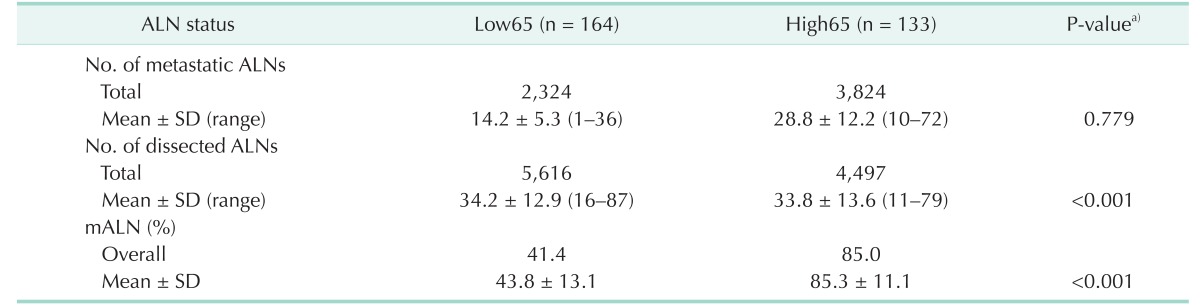
The total numbers of metastatic and dissected axillary lymph nodes of the 297 patients were 6,148 and 10,113, respectively. The overall mALNR (total metastatic axillary nodes/total dissected axillary nodes of the 297 patients) was 0.61. The mean (±standard deviation) number of metastatic axillary nodes was 20.7 ± 11.6 per patient (range, 1–72), and the mean number of dissected axillary nodes was 34.1 ± 13.2 per patient (range, 11–87). The mean numbers of metastatic and dissected axillary nodes were 14.2 and 34.2 in patients in the Low65 group (n = 164), respectively, and 28.8 and 33.8 in patients in the High65 group (n = 1,338) (Table 2).
Recurrence and survival rates according to mALNR
The 10-year overall survival rate of the 297 study patients was 52.6% (95% CI, 45.9–59.3).
The rates of recurrence (40.3% in Low65 group and 63.0% in high65 group) (including locoregional and systemic) were significantly different according to the mALNR (Table 1).
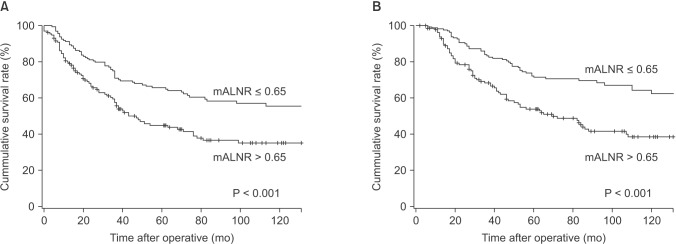
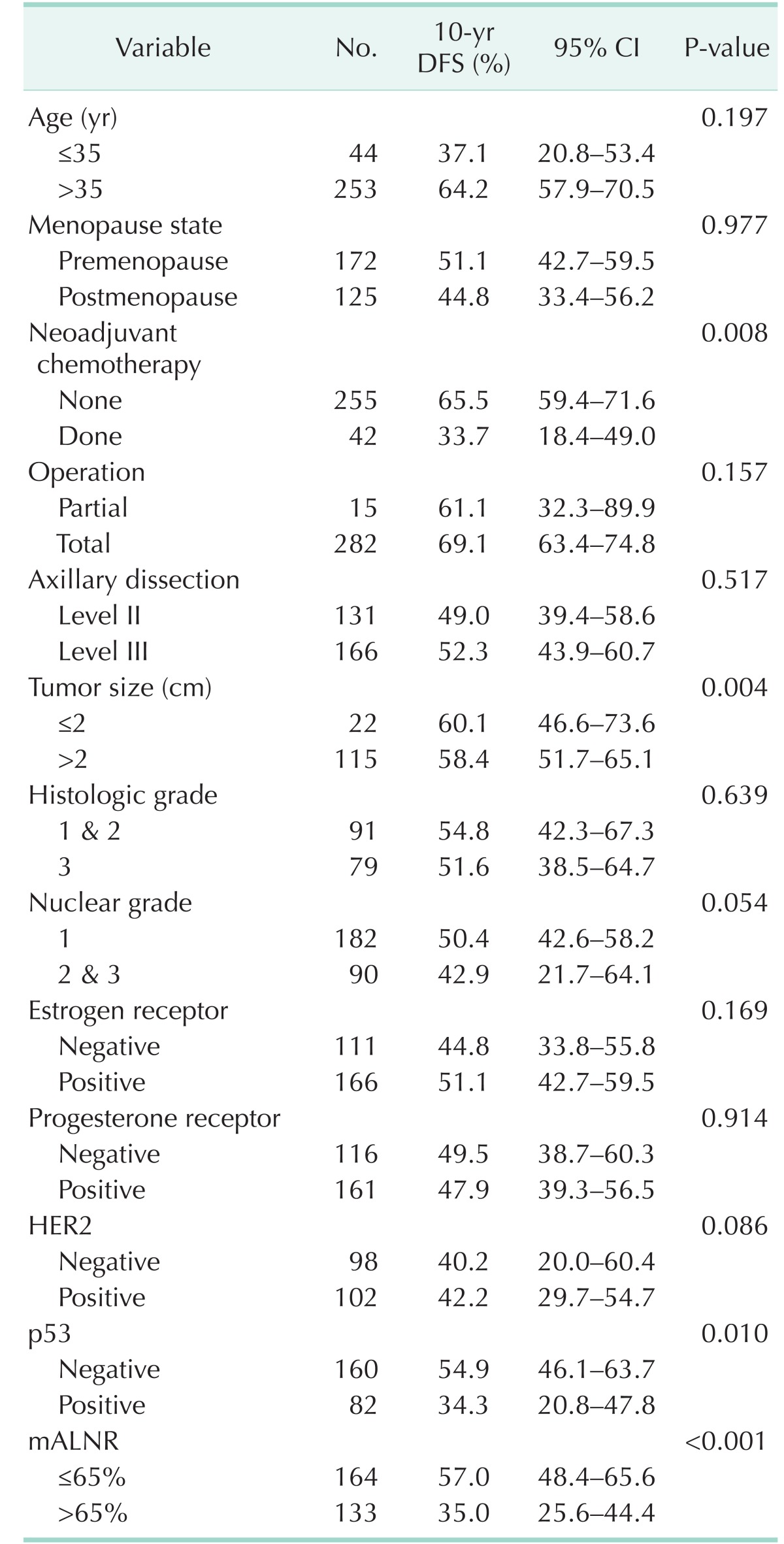
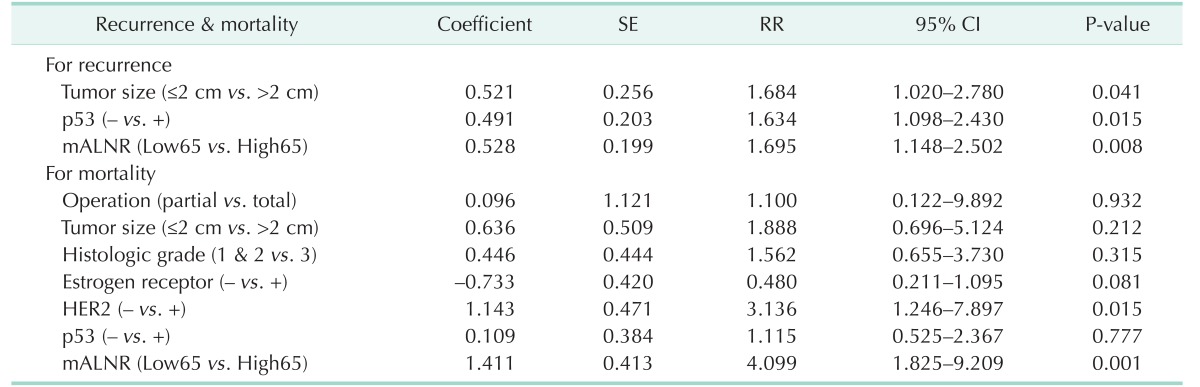
Univariate analysis for recurrence showed that neoadjuvant chemotherapy, tumor size, p53, and mALNR were significant predictors of disease-free survival (Table 3). The 10-year disease-free survival rate was 57.0% for the Low65 group and 35.0% for the High65 group (P < 0.001). Univariate analysis for mortality showed that operation (P = 0.038), tumor size (P = 0.007), histologic grade (P = 0.017), nuclear grade (P = 0.001), ER (P = 0.007), Her2 (P < 0.001), p53 (P = 0.016), and mALNR (P < 0.001) were significant predictors of overall survival (Table 4). The 10-year overall survival rate was 64.2% for the Low65 group and 38.3% for the High65 group (P < 0.001).
Multivariate analyses of recurrence and mortality
Multivariate analysis using the Cox proportional hazards model included prognostic parameters that were significant on the univariate analysis. Tumor size (P = 0.041), p53 (P = 0.015), and mALNR (P = 0.008) were independent prognostic factors of 10-year disease-free survival on multivariate analysis (Table 5). Her2 (P = 0.015) and mALNR (P = 0.001) were independent prognostic factors of long-term overall survival on multivariate analysis (Table 5). mALNR was the most significant and independent poor prognostic factor on multivariate analysis. Survival curves according to mALNR are shown in Fig. 1.
DISCUSSION
Stage IIIC breast cancer is generally associated with a poor prognosis (5-year survival rate of 40%) [316171819]. This study found long-term, 10-year disease-free and overall survival rates of 44.5% and 52.6%, respectively. These high survival rates might be due to the aggressive adjuvant treatment, including chemotherapy, endocrine therapy, and targeted therapy, performed in all eligible patients. For example, patients with HER2 positive breast cancer diagnosed before 2009 did not receive Trastuzumab because it was not covered by Korean insurance. Additional optimal targeted therapies, such as trastuzumab administration on the basis HER2 status, might be needed to improve clinical outcomes in patients with stage IIIC breast cancer [1].
In this study, young age (≤35 years) showed a tendency related to poor prognosis in both recurrence and mortality. Young age might have prognostic significance in advanced breast cancer. However, when examining increased age, menopausal status was not shown to be related to prognosis in this study.
Recently, many studies have suggested that mALNR can predict prognosis more precisely, and that mALNR should be incorporated into the next version of the staging system, regardless of the number of metastatic axillary nodes (based AJCC TNM breast cancer staging system) [12]. Several studies have reported that a significant cutoff value of mALNR for breast cancer is about 0.5–0.7 [13]. This cutoff value is useful for the prediction of recurrence and mortality. In this study, the most significant difference in locoregional and systemic recurrence was identified when 0.65 was used as a cutoff level. Further validation of this cutoff value is required.
When examining the results of our study, it is clear that the mALNR is not only the most significant prognostic factor, but also a useful tool for risk-stratifying patients with stage IIIC cancer. This finding is very important because most patients with more than 9 metastatic axillary nodes are categorized as pN3 disease. However, in our study, patients classified based on this nodal staging system did not have similar prognoses. Thus, this classification system might not be ideal for risk stratification of patients. In our study, when the cutoff value of the mALNR was set at 0.65, 164 patients has mALNR ≤0.65 and 133 >0.65. The 10-year disease-free survival rate was 57.0% and 35.0%, respectively. Among our patients, the recurrence rate was significantly different between the two groups: 40.3% vs. 63.0%, respectively (P < 0.001). This indicates that a substantial proportion of patients classified as having the same pN3 stage will experience recurrence after radical surgery, and that mALNR can be a better predictor of recurrence than the current TNM stage.
As shown above, high mALNR appeared to be a significant prognostic factor in both disease-free survival and overall survival. As reported in previous studies, maximal axillary dissection is recommended in breast cancer patients with advanced axillary nodal metastasis [1320]. Our study also found that mALNR was most significantly related to prognosis including recurrence and mortality. The metastatic lymph node ratio in other various cancer types is also thought to be an independent prognostic factor [212223]. Similar to previous studies, we found that a higher mALNR was associated with poor long-term prognosis in breast cancer.
The high rate of recurrence in patients with a high mALNR emphasizes the importance of aggressive adjuvant treatment. This importance was recently emphasized in several studies [152425]. These studies reported reduction in locoregional and systemic recurrence and increase in disease-free survival with adjuvant regional radiotherapy. This suggests that adjuvant radiotherapy is an essential treatment component in advanced breast cancer patients with axillary metastasis. The incidence of locoregional recurrence in our study was 12.8% (35 of 273), which is comparable with previous reports [2151926]. Even with multimodality treatment, a considerable proportion (approximately 5%–13%) of patients still experience locoregional recurrence [2151926]. In our study, high mALNR was the most important predictor of locoregional recurrence.
Several inherent limitations of this study should be described. First, it is possible that unrecognized biases might influence the results because of this retrospective study. Second, the specific sub analysis according to variable clinic-pathological parameters cannot be considered definitive, especially for the target anti-HER2 therapy (Trastzumab). Third, recent researches about lymph node ratio have been limited because there is no clear consensus about the cutoff points and many researchers have therefore used their own criteria. Therefore, further studies and follow-up are needed.
In conclusion, stage IIIC breast cancer is a disease with significant variation in long-term prognosis. The mALNR might serve as a more valuable prognostic indicator for patients with stage IIIC breast cancer than the traditional TNM stage. A high mALNR was the most significant independent prognostic factor influencing long-term prognosis including disease-free and overall survival. Furthermore, in patients with a high mALNR, aggressive adjuvant treatment and close follow-up might be required.
 XML Download
XML Download