

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Adherence, or compliance, is an essential aspect of effective healthcare delivery. However, non-adherence is a worldwide problem. Adherence in long-term therapy for chronic illnesses in developed countries is estimated at 50%, while the rate is even lower in developing countries.1 Adherence is important for a number of reasons, including improved healthcare outcomes, decreased healthcare costs and enhanced patient safety. It is also an important modifier of health system effectiveness. It has even been suggested that increasing the effectiveness of adherence interventions may have a much greater impact on population health than any improvement in specific medical treatments.2
Improving adherence in asthma therapy can be especially challenging for a number of reasons. In general, improvements in short-term treatment (<2 weeks) adherence can often be achieved by giving clear instructions, while long-term therapeutic regimens require a combination of clear and detailed instructions, counseling on the importance of adherence and how to best organize daily dosages, reminders about appointments and adherence, a reward system for the patient's successful adherence (especially important in children), and the support of family and friends.3 More specifically, asthmatic patient and caregiver education and self-management have been shown to be tremendously beneficial, while non-comprehensive approaches to asthma management, such as providing information only, have not demonstrated improvements in health outcomes.4
This study was the first nationwide survey of young asthmatic patients and caregivers in Korea that aimed to investigate adherence in 3 common asthma therapy delivery systems (i.e., inhaled or oral corticosteroids or transdermal β2-agonist) and identify possible reasons for nonadherence.
MATERIALS AND METHODS
Participants
Participants in this study were 2,000 asthmatic patients currently receiving treatment in the form of inhalant use or oral intake or transdermal patch for mild to moderate asthma. Twenty healthcare facilities (secondary or tertiary hospitals) belonging to the Korean Academy of Pediatric Allergy and Respiratory Diseases (KAPARD) participated. The participating hospitals were as follows: Catholic University of Korea Bucheon St. Mary's Hospital (n = 100, 5.44%); Kangbuk Samsung Hospital (n = 100, 5.44%); Kyongpook National University Hospital (n = 105, 5.71%); Kyunghee University Hospital (n = 103, 5.6%); Daegu Catholic University Medical Center (n = 98, 5.33%); Dong-A University (n = 101, 5.5%); Rosemary's Hospital (n = 106 5.77%); Busan National University School of Medicine (n = 100, 5.44%); Inje University Sanggye Paik Hospital A (n = 99, 5.39%); Seoul National University Hospital (n = 100, 5.44); Asan Medical Center (n = 102, 5.55%); Soon Chun Hyang University Hospital Cheonan (n = 99, 5.39%); I Dream Place Children's Hospital (n = 55, 2.99%); Catholic University of Korea Uijeongbu St. Mary's Hospital (n = 99, 5.39%); Inje University Busan Paik Hospital (n = 54, 2.94%); Inha University Hospital (n = 30, 1.63%); Presbyterian Medical Center (n = 33, 1.8%); Good Gang-an Hospital (n = 53, 2.88%); and Hanyang University Medical Center (n = 101, 5.5%).
Because asthma is a heterogeneous disease and especially difficult to diagnose in this age group, the definition of asthma used was based on the GINA guidelines. The major inclusion criteria were: 1) 3 or more recurrent wheezing episodes within the last year, with at least 1 confirmed by a physician, and multiple-trigger wheeze (not just the common cold but other triggers, such as exercise, crying, laughing, etc.;) and 2) improvement of wheezing after administration of inhaled or oral short-acting β2-agonists.
For severity, the GINA symptom classification based on daytime symptoms, nighttime symptoms and exertional symptoms was used. All patients were classified as having mild to moderate asthma.
Administration and contents of the questionnaire
This questionnaire-based study was carried out from March 2010 to February 2012. While visiting the clinic or hospital, asthmaic patients and their caregivers were given the questionnaire and they completed it on the spot or at home then mailed it in. The questions and answers are detailed in Table 1. Questions concerning sex, age, and underlying disease and severity were also included.
Table 1
Questionnaire

Medication
The tulobuterol patch (TP) is a transdermal patch containing the long-acting β2-agonist (LABA), tulobuterol. It is designed to exert sustained β2-agonist effects for 24 hours when applied once daily. The TP has been shown to improve lung function.5
Inhaled medication included: dry powder inhaler long-acting β2-agonist (DPI-LABA); metered-dose inhaler short-acting β2-agonist (MDI-SABA); DPI-inhaled corticosteroids (DPI-ICS); MDI-ICS; Budecort respules (aqueous solution of budesonide, an ICS); and Ventolin nebules (nebulized salbutamol, a SABA).
Oral medication included: leukotriene receptor antagonists (LTRAs), Montelukast and Pranlukast; oral corticosteroids (OCS); Theophylline; and Formoterol.
Statistical analysis
Using SPSS software, answers regarding adherence to treatment, convenience and willingness to replace drug formulation were analyzed using the Mann-Whitney U test. Answers regarding reasons for poor adherence were analyzed using the Z-test for comparisons inhaled, oral, and transdermal drugs. Sex proportions were analyzed using the χ2 test, while age was analyzed using the Wilcoxon rank sum test. The level of statistical significance was set at P < 0.05.
RESULTS
Demographics
A total of 1,838 patients completed and returned the questionnaire. Six hundred ninety-seven females (mean age, 5.93 ± 3.89 years) and 1,124 males (mean age, 6.00 ± 3.71 years) responded at an overall mean age of 5.98 ± 3.79 years, while 17 responders did not answer the sex question. There was no significant difference in age between females and males (Wilcoxon rank sum test; P = 0.511); however, there was a significant difference in sex proportion (χ2 test; P < 0.001).
The number of participants from each healthcare center and proportion of the total are listed in the Methods section. These amounts differed significantly (P < 0.001).
Questionnaire
Question 1 asked, “Are you currently taking medication prescribed for asthma treatment as directed by your physician?” Comparing the 3 types of medications in Table 2, 38.04% of inhalant users, 50.09% of oral users and 67.42% of TP users answered, “Always taken as prescribed.” These 3 proportions significantly differed (P < 0.001). Within each group, the proportions that answered, “Always taken…”, “Sometimes failed to take…”, “Frequently failed to take…”, or “Always failed to take…” also significantly differed (χ2 test; P < 0.001) (Fig. 1).
Table 2
Ease of medication use

Fig. 1
Adherence. Answers to Question 1, “Are you currently taking all asthma medications as prescribed?”

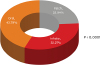
Question 2 asked, “What is the most commonly prescribed medication during the 6-month study period?” Referring to Fig. 2, 23.94% (n = 451) answered, “Patch”, 32.27% (n = 608) answered “Inhaler” and 43.79% (n = 825) answered “Oral”. The Rao-Scott χ2 test was performed and the above 3 proportions differed significantly (P < 0.001).
Fig. 2
The most common medication prescribed. Answers to Question 2, “What is the most commonly prescribed medication during the 6-month study period?”
Question 3 asked “Please rate the convenience of use of your asthma drugs using the following rank scale.” Referring to Table 2, 34.15% of inhalant users, 70.33% of oral medication users and 93.00% of TP users felt that their medication delivery system was “Easy” or “Very easy” to use. These 3 proportions differed significantly (P < 0.001). Within each group, the proportions that answered “Difficult”, “Slightly difficult”, “Easy”, or “Very easy” also differed significantly (P < 0.001).
Question 4 asked “Which part of the treatment regimen was difficult to follow?” Of the 1,767 selected answers, 719 (40.80%) were “Method of administration”; 510 (28.86%) were “Frequency of administration”; 401 (22.69%) were “Time”; and 135 (7.64%) were “Others”. There was a significant difference between the 4 answers (P < 0. 001). Three respondents selected more than 1 answer and 74 of the 1,838 total patients enrolled in this study did not respond to the question.
Question 5 stated “Please indicate the most preferable frequency of administration for your asthma drugs.” Of the 1,830 patients who responded to the question, 1,404 (76.72%) selected “Once daily”; 379 (20.71%) selected “Twice daily”; and 47 (2.57%) selected “Three times daily”. These 3 proportions differed significantly (P < 0.001). Eight patients did not respond to the question.
Question 6 asked “Who usually administers the drugs to the patient?” Of the total 1,825 responses to the question, 1,292 (70.6%) were “Mother or Father”; 229 (12.51%) chose “Grandmother or Grandfather or relative”; 28 (1.53%) chose “Family helper”; and 281 (15.36%) were “Self-administered”. These 4 proportions differed significantly (P < 0.0001). Five respondents selected more than 1 answer and 13 of the total patients enrolled in this study did not respond to the question.
Question 7 asked “Would you switch from inhaled medication to transdermal patch?” Of the 1,656 patients who responded to this question, 493 (29.77%) responded “Definitely yes”; 467 (28.20%) responded “Probably yes”; 495 (29.89%) responded “Do not know”; 114 (6.88%) responded “Probably no”; and 87 (5.25%) responded “Definitely no”. These 5 proportions differed significantly (P < 0.0001). Of the total patients enrolled, 182 did not respond to the question (Fig. 3A).
Fig. 3
Medication preference. (A) Inhalant users were asked, “Would you switch from inhaled medication to transdermal patch?” (Question 7). (B) Transdermal patch users were asked “Would you switch from transdermal patch to inhaled medication?” (Question 8).

Question 8 asked “Would you switch from transdermal patch to inhaled medication?” Of the 1,634 patients who responded to the question, 76 (4.65%) chose “Definitely yes”; 117 (7.16%) chose “Probably yes”; 577 (35.31%) chose “Do not know”; 531 (32.50%) chose “Probably no”; and 333 (20.38%) chose “Definitely yes”. These 5 proportions differed significantly (P < 0.001) (Fig 3B).
DISCUSSION
Overall, the results obtained from this questionnaire-based survey of young children with mild to moderate asthma and their caregivers were expected. Due to the nature of the 3 different therapy delivery systems (i.e., inhalant use, oral intake and transdermal patch), adherence was highest in the TP group and significantly greater than in the other 2 groups. This result is congruent with those obtained by previous studies of asthma medication adherence. Tamura and Ohta6 found TP users to be significantly more likely to take their medication as prescribed than inhalant users (84% vs. 31.0%-64.6%). The reasons for higher adherence in our study may be elucidated by the other questions contained in our questionnaire. The ninety-three percent of our respondents found the TP to be convenient, which may be due to factors such as the frequency of administration (once per day) and the drug effect period (lasts for 24 hours). This led to nearly 60% of respondents stating they would switch from inhaled medications to TP.
Since its introduction in 1998, the TP-LABA has been used extensively in Korea, Japan and China; consequently, it has demonstrated clinical efficacy and safety. It is also associated with improvements in quality of life (QOL) for asthma and other chronic respiratory disease (e.g., chronic obstructive pulmonary disorder [COPD]).7 Beyond these attributes, however, are the benefits due to its specific formulation and delivery system for a bronchodilator. As the human body follows circadian rhythms, respiratory function is known to be most compromised from late night to early morning.8 Suppression of this “morning dip” in respiratory function would logically improve QOL, and in the case of childhood asthma also reduce burden on the caregiver(s). This particular TP maximizes blood drug concentration in the early morning and provides a sustained drug action for 24 hours. In a small study of pediatric patients with severe asthma and being treated with ICS, the once-daily TP exhibited an add-on effect equal to twice-daily doses of inhaled salmeterol, another LABA.9
Treatment adherence is a critical factor in the management of chronic disease and is especially true for asthma. There is documented worldwide poor adherence in asthma treatment (30%-70%), with percentages being measured a number of ways: percentage of prescribed medication taken, serum theophylline levels, days of medication adherence or percentage of patients who failed to reach a clinically estimated adherence minimum.10 Adherence is also a serious consideration in vulnerable populations like children and adolescents, and has been measured as low as 30% in general practice.11 The importance of asthma treatment adherence cannot be overstated, as it not only has direct health consequences – for example, poor asthma control leading to exacerbation and decreased QOL – but also economic costs such as increased hospitalization and emergency department visits.1
One possible limitation of our study is the fact that caregivers often answered the questionnaire for young children. Measurement bias may have occurred because caregivers may have been reluctant to give socially unacceptable answers to questions regarding adherence. Another possible limitation may have been in the sex ratio (i.e., almost 2:1 for male:female. However, males tend to be afflicted by asthma more often than females.
Continued improvement in treatment adherence for chronic diseases such as asthma should be the focus of all practicing clinicians. Consistent administration of effective doses at the correct times is essential for asthma control, which is the goal of every healthcare personnel and caregiver dealing with this disease.
 XML Download
XML Download