

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is an inflammatory disorder of the lungs causing the airways to swell and narrow, shortness of breath, chest tightness, and coughing. Asthma is estimated to affect 300 million people worldwide, with a prevalence ranging from 1%-18% across different countries.1 The prevalence of asthma is comparatively low in the Asia-Pacific region, with a value of 3.9% reported for South Korea in 2004.2 However, asthma prevalence is increasing in South Korea, such that values of 7.8%-17.7% were reported in 2009 for adults of various ages.3
Among the factors influencing the onset and course of asthma are environmental agents including allergens, air pollution, and tobacco smoke.1 There is evidence that exposure to environmental tobacco smoke may both cause adult-onset asthma and worsen existing asthma symptoms in non-smokers.4 Active smokers with asthma have poorer symptom control than non-smokers,5 arising perhaps from increased inflammatory markers at the cellular level and/or a greater degree of airway remodeling.6 Studies of the Cohort for Reality and Evolution of adult Asthma in South Korea ('the COREA cohort') support this assertion. The COREA cohort indicated that smoking was associated with a history of exacerbation and more exacerbation-related physician visits.7 In subgroup analyses at year 1 of those with severe asthma, a longer duration of smoking (≥5 pack-years versus <5 pack-years) was associated with fixed airway obstruction.8 Asthma patients who smoke are also less responsive to treatment with corticosteroids, as demonstrated by randomized controlled clinical trials in Europe9,10,11 and the United States.12 Possible mechanisms for this effect include overexpression of the nonfunctional glucocorticoid receptor β subtype in smokers6; reduction of histone deacetylase-2 activity, presumably caused by cigarette smoke leading to increased expression of inflammatory genes6; an increase in neutrophil-mediated inflammation, which improves upon smoking cessation13; and increased leukotriene production.14
In South Korea, 29.1% of the general population smokes-52.8% of men and 5.8% of women.15 Because smoking is so common in South Korea, and because of its detrimental effects on asthma patients' symptom control and response to treatment with corticosteroids, we sought to determine the prevalence of smoking in Korean asthma patients and to compare the asthma medications among those who do and do not smoke.
MATERIALS AND METHODS
Study design
A cross-sectional survey was conducted from August 2010 to January 2011 (the study period) at 16 urban study sites across South Korea. Physicians recorded demographic and clinical data on all asthma patients presenting during the study period and then recruited a subset of asthma patients for participation in the study. Physicians completed a questionnaire for each study patient using the patient's medical records. Each study patient completed a questionnaire during the study visit. Questionnaires were approved by the ethics committees of Hallym University Sacred Heart Hospital and Ajou University Hospital. The study was also registered with the Korean Research-based Pharmaceutical Industry Association (KRPIA). Patients provided informed consent for study enrollment.
Study sample
Participating physicians were qualified after 1965, were personally responsible for treatment decisions for patients with asthma, saw >5 patients with asthma who smoke per week, and were willing to consent to participate for the duration of the study. Twenty-five physicians from 16 study sites located in 6 South Korea cities (8 sites each in Seoul and Gyunggi provinces) completed a log of the first 40 asthma patients presenting, regardless of smoking status or participation in the study. This non-identifying data was used to estimate the prevalence of smoking in the general asthma patient population. The physicians then recruited 10 smokers and 10 non-smokers each, resulting in a study population of 250 asthma patients who smoked and 250 asthma patients who did not smoke. The majority of participating physicians (84.0%) worked in hospitals, whereas the rest (16.0%) worked in clinics.
The study population included asthma patients between aged 18-60 who, upon recruitment by the physician, agreed to complete the patient questionnaire in their local language. Patients were excluded if they had a diagnosis of chronic obstructive pulmonary disease, bronchiectasis, bronchiolitis, cystic fibrosis, lung cancer, or pneumonia; had an infection or condition of the airway other than asthma; had limited cognitive functioning; or had participated in a clinical trial related to asthma in the previous 6 months. Both physicians and patients were compensated for their participation.
Questionnaires
The physician questionnaire included physician-recorded, patient-specific information on demographics, clinical evaluation, smoking history (current, former, or never), asthma medications, asthma-related consultation history, and comorbid conditions. The patient questionnaire recorded information on smoking history (current, former, or never), asthma symptoms, asthma treatment regimen, asthma-related resource utilization, and asthma control. Quality of life was assessed by the EuroQol (EQ)-5D (ref).
Study definitions
Frequency and history of smoking was used to categorize patients as a current smoker (frequent: >5 cigarettes a day vs infrequent: ≤5 cigarettes a day), a never-smoker, or a former smoker (someone who stopped smoking at least 6 months ago). Asthma-related resource utilization included planned and unplanned doctor visits, emergency care, and hospitalizations. The number of occurrences of each type of resource utilization was totaled over the previous 12 months. The number of exacerbations in the previous 12 months, defined as unplanned visits for an exacerbation or as emergency treatment or hospitalization for asthma, was self-reported by the patient.
The level of asthma control for each study patient was defined by the physician per the Global Initiative for Asthma (GINA) recommendations.1 Specifically, the physician survey contained the schema presented in the GINA guidelines for assessing asthma control. A determination of 'controlled' asthma required having daytime symptoms and needing rescue treatment less than thrice weekly; and having no nocturnal symptoms, no limitations in activities, and normal lung function. If daytime symptoms or need for rescue treatment occurred more than twice per week, or if any nocturnal symptoms or limitations in activities were present, or if lung function was <80% of the predicted or personal best value, then the patient's asthma was deemed 'partly controlled'. 'Uncontrolled' asthma was defined as having three or more characteristics of partly controlled asthma.
Asthma medication use was determined by the physician and used to define the treatment regimen for each patient. Medication regimens were classified as 5 'steps' according the GINA recommendations.1 At step 1, patients use a short-acting beta-agonist (SABA) as needed. The recommended add-on therapies at steps 2-4 are low-dose inhaled corticosteroids (ICSs), low-dose ICS plus a long-acting beta-agonist (LABA), and medium- or high-dose ICS plus a LABA, respectively. Step 5 incorporates the use of oral corticosteroids (OCSs) or anti-IgE treatment. The following adjustments were made to the treatment definitions to facilitate patient classification. Bambuterol and tulobuterol were defined separately from the other LABAs and not used for GINA classification. Ipratropium and tiotropium were excluded during the classification process. Chronic use of OCSs was classified as GINA Step 5. Acute use of OCSs was classified according to the other components of the medication regimen.
Statistical analysis
All statistical analyses were conducted using STATA SE v.12.1 (College Station, TX, USA). Power calculations showed that 250 smokers and 250 non-smokers were needed to detect a minimum difference of 12.4% in the use of asthma medications between smokers and non-smokers, assuming a two-sided alpha of 0.05, 80% statistical power, and a conservative estimate of 50% medication use among smokers. This power calculation applied to the original evaluation of potential differences in asthma medications between smokers and non-smokers and was not intended to test differences according to GINA treatment steps. A descriptive analysis of the patient population with regard to age, smoking status, rhinitis, medication use, and exacerbations was performed using data from the physician questionnaire. The Kappa statistic was computed to assess the level of agreement between the physician-determined and patient-reported smoking status. Clinical characteristics, asthma control, healthcare resource utilization, and quality of life were assessed descriptively according to patient-reported smoking status. Finally, asthma medication regimens (defined by the five GINA steps) and quality of life (i.e., the mean EQ-5D visual analog scale [VAS] scores), were assessed according to patient-reported smoking status. P values for proportional distributions were calculated using Fisher's exact tests or chi-square analyses, and those for mean VAS scores were calculated with ANOVA or t-tests.
RESULTS
Participants
The characteristics of all asthma patients presenting during the study period and patients participating in the study are shown in Table 1. Current smoking was recorded for 17.3% of patients in the presenting population, former smoking for 19.2%, and never smoking for 63.5%. Among the 500 patients recruited for the study, 28 had data that could not be linked to the original physician record and one had missing data on smoking status, leaving an analyzable study population of 471. Patients in the study population were younger on average than all presenting patients (43.4 vs 52.0 years) and, because of the study selection criteria, smoking was much more frequent in the study population (48.0%; Table 1). Concomitant rhinitis was common in both groups (67.7% in the study population and 58.8% in presenting patients), and the most frequently used asthma medications in both the study and presenting populations were ICS/LABA fixed-dose combinations (78.3% and 74.9%, respectively), anti-allergic drugs (60.7% and 51.1%, respectively), and leukotriene modifiers (52.4% and 50.8%, respectively).
Physician-patient agreement on smoking status
Within the study population, 212 patients reported smoking currently, 79 smoking formerly, and 180 never smoking (Table 2). Correlation between physician-reported and patient-reported smoking status was strong (κ=0.82; P<0.001). The most common mismatch was among physicians designating self-reported former smokers as current smokers or never smokers.
Patient characteristics by smoking status
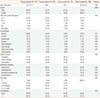
Patient characteristics according to smoking status (Table 3) revealed substantial differences between men and women in smoking behavior. The study population comprised 56.9% men, but among current and former smokers, 79.7% and 81.0%, respectively, were men. Conversely, while 43.1% of the total study population was female, women represented 80.5% of patients who had never smoked.
Current and never smokers had similar patterns of asthma duration, comorbidities, and asthma control. Certain types of healthcare resource utilization differed numerically, though not statistically significantly, by smoking status (Table 3): 26.1% of never smokers (compared to 16.5% of current smokers) had an unplanned visit during the previous year, and 12.2% of never smokers had been hospitalized (compared to 6.6% of smokers). In addition, 47.2% of never smokers had ≥ 1exacerbation during the previous year compared to current and former smokers (36.3% and 36.7%, respectively).
Asthma medication regimen and quality of life by smoking status
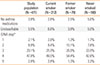
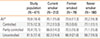
There were no statistically significant differences in asthma medication regimen between smoking and non-smoking asthma patients (Table 4). Mean quality of life scores by smoking status are shown in Table 5. Mean VAS scores increased with increasing asthma control in the combined study population (P<0.001) across all smoking categories. Quality of life did not differ by smoking status in the combined study population (P=0.23), though never smokers with uncontrolled asthma had a numerically lower mean quality of life score (58.7) than current and former smokers with uncontrolled asthma (62.3 and 66.9, respectively).
DISCUSSION
This cross-sectional study examined smoking status and medical treatment among asthma patients presenting for medical care at clinical practice sites in South Korea. The prevalence of current smoking in the presenting population was 17.3%, somewhat lower than the value of 26.6% found in the Korean NHANES survey,16 but close to that reported in the Asthma Insights and Reality in Asia-Pacific study: 19.6% for Korea, 19.1% overall.17
The significantly greater proportion of male asthma patients who are current smokers, compared to female asthma patients, is consistent with statistics from the World Health Organization for the general population15 suggesting that a more intense need for smoking cessation exists among the former group. Community-wide18 and individual19 efforts at smoking cessation have proven to reduce asthma-related resource utilization and improve lung function.
Despite the higher prevalence of smoking among men, women in this study had higher odds of having partly controlled or uncontrolled asthma than men (OR 1.46; 95% CI 0.64-3.31) in multivariate logistic regression analyses (not shown), although not statistically significant (P=0.37). The prevalence of current smoking among female asthma patients in this study (20.3%) was much higher than that reported for the general population (5.8%)15 or in previous studies of asthma patients (4.9%).20 Korean women may feel they need to hide their smoking status, since smoking by women is not well accepted in Korean society, but may be more comfortable revealing their smoking status to a physician.
This study revealed that physicians in Korea have a very good awareness of the smoking behaviors of their asthma patients and hence could make appropriate therapy selections based on the patients' smoking status. However, no statistically significant differences were observed in the treatment regimens prescribed, suggesting that physicians make treatment decisions based on clinical characteristics other than smoking status. Neither asthma control nor quality of life differed across smoking status. Similarly, Jang et al.19 reported equivalent improvements in quality of life in smokers and quitters receiving inhaled fluticasone propionate in a small study of asthma patients recruited from Soonchunhyang University Bucheon Hospital in Korea.
Smoking has been shown to decrease the responsiveness of asthma patients to ICSs9,10,12,21 and the relationship between ICS dose and level of smoke exposure.23 Previous studies indicated up to 56% of asthma patients in Korea are prescribed ICSs,17,22 and 83.5% of the current study population used them, either alone or in combination with LABAs. Alternative therapies (i.e., leukotriene modifiers) are available, but clinical trials are needed to establish their efficacy in asthma patients who smoke.6 Future observational studies could assess the usage patterns of alternative treatments in asthmatic smokers and compare the respective levels of asthma control to those of non-smokers.
The current study provides valuable information on how physicians in Korea treat asthma patients who smoke, yet several limitations exist. First, it is likely that consulting bias affected the study outcomes. Patients seeking medical care are more likely to be poorly controlled and uncontrolled than patients not consulting. Also, the relationship between smoking and treatment regimen may have been confounded by the high frequency of prior exacerbations in both smokers and non-smokers, which suggests equivalent levels of asthma severity. The study was powered to detect differences in asthma medication regimens rather than GINA treatment step, which may have hindered detection of statistical significance in the differences in treatment step distributions among the smoking subgroups. Finally, because the study was designed to include approximately equal numbers of smoking and non-smoking patients, the comparisons between the groups may not fully reflect the distinctions between smokers and non-smokers in the general asthma patient population. Physicians and patients involved in this study may not be representative of care provided for all asthma patients in South Korea given the involvement of only 16 clinical sites in South Korea.
In conclusion, this study showed that in South Korea, physicians' assessments of smoking status agree well with patients' self-reports, allowing them to make appropriate therapy selections. However, medication regimens did not differ between smokers and non-smokers, suggesting that physicians make treatment decisions based on factors other than smoking status. Physicians' consideration of the patients' complete clinical profile, including smoking status, and need for medical care will adequately inform the need for higher-step therapy or alternative agents.

 XML Download
XML Download