

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is characterized by variable airflow obstruction, bronchial hyperresponsiveness (BHR), and airway inflammation.1 In general, bronchial challenge tests (or induced sputum analysis) are applicable to assess BHR or underlying lung inflammation2,3,4; however, the tests can be invasive as well as require specialized instruments and personnel.5
Nitric oxide (NO) is a gaseous molecule released by the human respiratory tract and increases under airway inflammatory conditions.6,7,8,9,10,11 Exhaled NO correlates well with eosinophilic airway inflammation and BHR12 and its measurement is safe.5,14,15 Current American Thoracic Society (ATS) guidelines recommend the use of the fraction of exhaled NO (FeNO) and induced sputum analyses to diagnose eosinophilic airway inflammation.7
Exhaled NO levels are influenced by various demographic factors13,14; therefore, the reference range for clinical applications should be specifically determined for the population. Kim et al. previously reported on FeNO reference ranges in Korea; however, the results were derived from relatively small-sized and younger adults (n=166; mean age, 32.7 years).15 In this context, the present study investigated FeNO reference ranges and determinants using the Ansung cohort dataset (a prospective community population cohort) in Korea.
MATERIALS AND METHODS
Study population
Study participants were recruited from the Ansung cohort. The design of this cohort and methods used have been previously described.16 The Ansung cohort was established for the Korean Health and Genome Study in 2001 to investigate the frequency and determinants of chronic diseases in Korea. Participants included residents in a rural area 100 km south of Seoul. Sampling was based on mailing and door-to-door/telephone interview in 5 randomly selected governing regions.
From the 1,730 Ansung cohort participants, the present study initially analyzed 997 subjects who underwent NO measurement in 2011. The subjects were asked to answer structured questionnaires on medical history and allergic symptoms. Subjects underwent chest X-ray, spirometry, methacholine bronchial challenge tests, and allergen skin prick tests. The focus of the investigation was on reference ranges for healthy adults; therefore, we excluded individuals: (1) under 18 years old, (2) current smokers, (3) a previous diagnosis of allergic diseases (asthma, allergic rhinitis, atopic dermatitis, or chronic urticaria), (4) recent infections (within the past 3 weeks), (5) underlying lung diseases (bronchiectasis or chronic bronchitis) identified by questionnaire or chest X-ray, (6) current use of inhaled or systemic corticosteroids, (7) airway obstruction (defined by prebronchodilator forced expiratory volume in 1 second [FEV1] % predicted <80%), or (8) BHR (methacholine PC20 <16 mg/mL). Study procedures were in accordance with institutional guidelines and approved by the institutional review board of Seoul National University Hospital. Informed consent was obtained from each participant.
Fraction of exhaled NO measurement
FeNO was measured using an online nitric oxide monitor (NIOX MINO, Aerocrine, Sweden) according to 2005 ATS/ERS guidelines.13 The subjects were asked about current medication or food intake that could interfere with the FeNO measurement results. In addition, they were instructed to avoid smoking, exercise, and ingestion of food, water or, caffeine at least 1 hour before testing.
The subjects exhaled fully while seated. The patient then inhaled over 2 to 3 seconds to total lung capacity through a NIOX filter and exhaled with an upper airway pressure of 5 to 20 cm H2O. FeNO measurements were taken from a stable plateau of the exhaled NO concentration of at least 3 seconds during exhalation. The lowest detection limit of NIOX MINO was 5 parts per billion (ppb), and values less than 5 ppb were considered 2.5 ppb. The average levels of at least 2 acceptable measurements were used.
Spirometry and methacholine challenge test
Pulmonary function was measured using a spirometry after FeNO measurement. The predicted values of FEV1 were calculated on the basis of the Morris method.17 Methacholine challenge tests were performed using a 5-breath protocol with a dosimeter.18 Methacholine dilutions of 1, 4, 8, and 16 mg/mL were used. Spirometry was performed 30 seconds and 90 seconds after each inhalation. The test was finished when FEV1 decreased by more than 20% from the baseline. A provocation concentration that caused a 20% decrease of FEV1 was defined as the provocation concentration dose for methacholine (PC20). BHR was defined as PC20 <16 mg/mL.
Skin prick test
An allergen skin test was performed using 12 common inhalant allergens in Korea: Dermatophagoides pteronyssinus, Dermatophagoides farinae, Alternaria tenuis, Aspergillus fumigatus, cockroach, cat, dog, early blossoming tree pollen mix (alder, hazel, poplar, elm, and willow tree), late blossoming tree pollen mix (birch, beech, oak, and plane tree), grass pollen mix (grass, barley, oat, rye, and wheat), ragweed, and mugwort. A 0.9% sodium chloride solution and a 1 mg/mL histamine solution were used as negative and positive controls, respectively. The test was considered positive when an allergen wheal to histamine wheal ratio was 1 or greater. Atopy was defined as positive skin test responses to any of 12 allergens.
Recruitment of asthma patients
To validate the diagnostic utility of FeNO reference levels, asthma patients were recruited from medical institutions (Seoul National University Hospital, Seoul National University Bundang Hospital, Asan Medical Center, Hanyang University Hospital, Korea University Hospital, Eulji University Hospital, and Ajou University Hospital). Asthma was diagnosed by typical asthma symptoms and positive BHR or a positive bronchodilator response (increase in FEV1 of >12% predicted and 200 mL after inhalation of a short-acting β2 agonist). Enrolled asthma patients were not currently receiving asthma medications, such as corticosteroids or antileukotrienes.
Statistical analysis
Statistical analysis was performed using the SPSS software (ver. 19.0 for Window; SPSS, Inc., an IBM Company, Chicago, IL, USA). Data were presented as a number and percentage for categorical variables and mean ± SD for continuous variables. Comparisons between variables were performed by Pearson's chi-square test for categorical variables and by Student's t test for continuous variables. FeNO levels were not normally distributed; therefore, FeNO levels were log-transformed before analysis. Simple linear regression analysis determined the association of log-transformed FeNO (a dependent variable) with age, gender, weight, height, body mass index (BMI), atopy, and FEV1% predicted. Potentially relevant factors (with P<0.2 in simple linear regression analysis) were included in multiple linear regression analysis. The reference values of FeNO are presented as mean±SD, median and interquartile range (IQR), and 90% confidence interval (CI, 5th to 95th percentile). Receiver-operator characteristic (ROC) analysis validated the diagnostic utility of FeNO from the combined group of healthy population and asthma patients. A P value less than 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
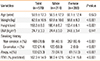
We included 570 subjects (mean age, 59.9±12.3; male, 37.0%) after excluding (n=427) subjects according to predetermined criteria (under 18 years old, n=12; current smoker, n=169; asthma, n=20; allergic rhinitis, n=96; atopic dermatitis, n=16; chronic urticaria, n=2; underlying lung diseases, n=3; current use of corticosteroids, n=4; airway obstruction, n=127; and BHR, n=13). Table 1 describes the baseline characteristics of the study subjects. Of the subjects, 133 (23.3%) had atopy, which was more frequent in males than females (P<0.001). Height and weight were greater in males, and FEV1 predicted values were higher in females; however, BMI did not differ.
Determinant factors and reference ranges
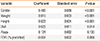
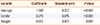
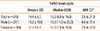
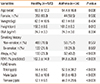
A simple linear regression analysis was performed to assess the association with age, gender, atopy, FEV1 predicted value, and anthropometric values (Table 2). Potentially relevant factors for FeNO (P<0.2) were gender, weight, height, BMI, atopy, and FEV1 predicted value; however, age was not a meaningful determinant. In multiple linear regression analysis with adjustment for relevant factors (P<0.2 in univariate tests), gender and weight were found to have significant associations with FeNO levels (Table 3). The intercept value was 1.546, and log-transformed FeNO increased by 0.376 in males compared to females when weight was assumed to be constant (P<0.001). The statistical significance for weight was not correlated to FeNO levels in individual gender groups and suggested a confounding effect with gender (data not shown); therefore, reference values and basic statistics were derived with gender as the determinant factor for FeNO levels (Table 4). FeNO reference ranges were 18.2±10.6 ppb in males and 12.1±6.9 ppb in females. The 90% confidence interval (5th to 95th percentile) was 6.0 to 37.4 ppb in males and 2.5 to 27.0 in females.
Utility of FeNO for the diagnosis of asthma
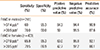
We compared the distribution of FeNO levels in asthma patients and healthy population to validate the utility of FeNO (Fig. 1); subsequently, the ROC curves were constructed from the combined group of 570 healthy population and 74 asthma patients (mean age, 54.4±16.8; male, 40.5%; Table 5). The area under the ROC curve was 0.900 in males and 0.885 in females (Fig. 2). The sensitivity and specificity of FeNo measurement was 60% and 95.3% respectively in males 65.9% and 95.3% in females when the cutoff value of FeNO for the prediction of asthma was provided from the upper limit of 90% CI (37.4 ppb for males and 27.0 ppb for females) (Table 6). The cutoff value from the best combination of sensitivity and specificity was 30.5 ppb in males and 20.5 ppb in females; this indicated a sensitivity of 70.0% and a specificity of 90.0% in males, a sensitivity of 79.5% and a specificity of 86.9% in females (Table 6).
DISCUSSION
The current analysis presented the FeNO reference range levels for healthy Korean elderly populations. We presented the gender-specific reference values of FeNO because gender was identified as a determinant factor; additionally, reference levels showed a good diagnostic utility for asthma diagnosis.
Our findings on gender association are consistent with those of previous reports15,19,20,21,22; however, mechanisms for the associations are unclear. A few hypotheses have been suggested in the literature. The first explanation is the effect of flow-induced dilution.23,24,25 The flow in small airways should be higher for the constant flow rate at the mouth level. FeNO would be lower in females with relatively smaller airways compared to males because exhaled NO is lower in a high flow.24 However, the limited reports on children indicate that FeNO levels correlate more significantly with age than gender.26,27 Age-dependency in children, not gender-dependency, may be related to increased lung volume and airway surface area development.27 The difference in airway size may explain that exhalation flow rate in young children is relatively higher. The difference in lung volume and airway surface area may also account for an association between FeNO levels and height or weight, which are generally greater in males. Therefore, the difference in airway surface area may be considered as a crucial reason for a gender-related difference.20,25 An age-relationship does not seem evident in adult populations,15,19,28 and the present analysis did not indicate an association between age and FeNO levels.
Atopy was not an independent determinant for FeNO levels in our study population in contrast to the results of previous studies.21,22,29 A previous study with the Korean population conducted by Kim et al.15 in indicated that atopy (alongside gender) is a significant predictor of FeNO levels. The difference in the 2 Korean studies is assumed to have originated from the study population characteristics. Age distribution was considerably younger in the study conducted by Kim et al. (mean age, 33.7 years) than in our study (mean age, 59.9 years). In addition, the varying prevalence of atopy may have affected the statistical power (48% in the study conducted by Kim et al. vs 23.3% in our study). The negative findings on atopy association need to be confirmed by further studies with older adult populations; however, our findings potentially indicate significance in determining population-specific reference ranges.
Previous literature has suggested that FeNO levels are higher in Asians than in other ethnic groups24,26,27 and accounted for dietary differences, such as salted and nitrate-rich meals or genetic variations of the NO synthase gene.24,30 However, the present analysis did not find higher FeNO levels in Korean adults as compared to Western populations.5,21,28 Kharitonov et al.5 prepresented mean FeNO of 17.8±6.8 ppb in a healthy adults study that demonstrated the reproducibility of FeNO for a healthy or asthma population in the UK (healthy adults n=10, age=35.6±9.39, non-atopy). Travers et al.21 suggested a mean FeNO of 17.9 ppb in healthy New Zealander adults (n=193, mean age=56.3±12.9, atopy rate=23.8%), and Olin et al.28 showed a FeNO level of 16.6 ppb in healthy Swedish adults (n=1,131; mean age, 50.3±13.81; atopy rate, 25.3%). In Asia, Chng et al.29 presented a median FeNO level of 38.4 ppb for atopic subjects and 15.7 ppb for non-atopic subjects in Singaporeans (n=45, mean age, 19.6; atopy rate, 61.8%); however, their subjects were younger than ours. We speculate that the reason for our lower FeNO ranges (than other ethnic groups) may be due to differences in living environment. Our study populations were from rural areas, were less likely to be exposed to pollutants that could influence airway inflammation and were at lower risk for asthma. It is well-known that living in rural areas exerts a protective effect on asthma or atopy,31,32,33 as suggested by the 'hygiene hypotheses'. The participants of previous studies were mostly recruited from urban areas.5,21,28,29
The relatively lower FeNO levels in our study could be related to inclusion/exclusion criteria. Previous studies did not exclude subjects with BHR; subsequently, their FeNO levels may have been affected by subjects with asymptomatic BHR.15,19,22
There are several limitations to our study. Our study population may not be representative of the entire Korean population. In particular, our participants were mostly older adult residents living in a rural area. In addition, the relatively low number of male subjects may have limited the statistical power and have resulted in the inclusion of ex-smokers. We did not match the age of the healthy population and asthma patients recruited to validate the utility of FeNO in the diagnosis of asthma because the number of asthmatic patients who underwent the FeNO measurement was small. However, age and a former history of smoking did not significantly correlate with FeNO levels. Despite the limitations, we expect our data to provide useful reference ranges for epidemiologic studies in elderly Korean adult populations. Recent literature suggests that asthma or allergic respiratory diseases are no longer childhood diseases34; subsequently, there is significant interest in epidemiologic surveys of asthma in an aged population.35,36,37 Our results are expected to be useful for older adult patients visiting medical institutions for asthma diagnosis as shown in ROC analysis.
In conclusion, we present FeNO reference ranges for healthy Korean elderly adults and a diagnostic utility for asthma.


 XML Download
XML Download