

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hyo-Joon Yang , In-Gu Do1, Chang Hak Yoo2
, In-Gu Do1, Chang Hak Yoo2
, In-Gu Do1, Chang Hak Yoo2
Figures and Tables
Fig. 1
Esophagogastroduodenoscopy findings. A large subepithelial tumor with a normal overlying epithelium larger than 5 cm in size occupying cardia and mid to high body lesser curvature side.

Fig. 2
Abdominal computed tomography (CT) and positron emission tomography (PET). CT images show (A) a 6.7 cm sized large mass arising from the left side of the gastric body (arrow) and (B) left paraaortic lymph node enlargement (arrow). PET images show increased 18F-fluorodeoxyglucose uptake in (C) left gastric mass and (D) left paraaortic lymph node.
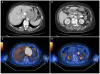
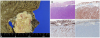
Fig. 3
Pathology findings of a fine needle aspiration/biopsy specimen. (A) Microscopic findings of the specimen show poorly differentiated small epithelioid cell nests (H&E, ×20). (B) Immunohistochemical staining findings were compatible with the diagnosis of a poorly differentiated carcinoma (upper left: CK [AE1/AE3], ×20; upper right: CD 56, ×20; lower left: LCA, ×20; lower right: Vimentin, ×20).

Fig. 4
Pathology findings of a surgical specimen. (A) Gross appearance of the resected stomach shows a gray white to pale yellowish solid mass involving the submucosa to serosa. The mucosa surface is intact. (B) H&E stain revealed intact mucosa and poorly differentiated small epithelioid tumor cells involving the submucosa to serosa (upper left: H&E, ×4). Tumor cells are positive for CK (AE1/AE3) and negative for LCA, CD56, and vimentin. Based on the H&E and immunohistochemistry findings, tumor is consistent with a poorly differentiated adenocarcinoma (upper right: CK [AE1/AE3], ×4; lower left: LCA, ×4; lower right: CD 56, ×4).
References
1. Umehara Y, Kimura T, Okubo T, et al. Gastric carcinoma resembling submucosal tumor. Gastric Cancer. 1999; 2:191–193.

2. Kim HI, Shim KN, Yoon SY, et al. A case of early gastric adenocarcinoma resembling subepithelial tumor. Korean J Helicobacter Up Gastrointest Res. 2013; 13:60–63.
3. Ohara N, Tominaga O, Uchiyama M, Nakano H. A case of advanced gastric cancer resembling submucosal tumor of the stomach. Jpn J Clin Oncol. 1997; 27:423–426.
4. Standards of Practice Committee. Faulx AL, Kothari S, et al. The role of endoscopy in subepithelial lesions of the GI tract. Gastrointest Endosc. 2017; 85:1117–1132.
5. Fujiyoshi A, Kawamura M, Ishitsuka S. Gastric adenocarcinoma mimicking a submucosal tumor: case report. Gastrointest Endosc. 2003; 58:633–635.
6. Yamane H, Ishida M, Banzai S, et al. Advanced gastric cancer with features of a submucosal tumor diagnosed by endoscopic ultrasound-guided fine needle aspiration and boring biopsy preoperatively: a case report and literature review. Int J Surg Case Rep. 2019; 55:223–226.
 XML Download
XML Download