

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Among all patients undergoing endoscopic ultrasound (EUS) for pancreaticobiliary indication, pancreatitis is an uncommon complication, reported only in 1–2% of all cases.12 EUS-guided biopsy of the pancreas can usually be performed avoiding the pancreatic duct (PD) and/or passing a needle through a significant portion of the normal pancreatic parenchyma, which might help decrease the rate of post-EUS fine needle aspiration (FNA) pancreatitis. It is also possible that some cases may go unnoticed due to milder clinical presentation or symptoms that can be confused with the underlying diseases, such as pancreatic cancer or chronic pancreatitis. Moreover, the nature of retrospective study also contributed to the under-reporting of this complication.3 It is accepted that when the needle traverses the normal parenchyma and/or PD, the rate of pancreatitis may be higher, although this concept is based on scarce data.4 Other factors have been shown to be associated with post-EUS pancreatitis; for example, patients with recent history of acute pancreatitis may be exposed to a greater risk or when FNA of side branchintraductal papillary mucinous neoplasm (IPMN) results in injury to nearby PD.45 In one of the first publications raising concerns about the sampling of normal parenchyma came from a 2015 case series in Indiana. The authors performed core biopsy of the pancreatic parenchyma using the Trucut design needle to determine the presence of chronic pancreatitis in 18 patients.6 One patient was admitted with abdominal pain and a second developed acute pancreatitis (1/18, 5.5%). Because of the limited diagnostic yield and higher complication rate, the authors recommended against core biopsy of the normal parenchyma in 2005. Since then, other reports confirmed that EUS FNA can result in severe acute pancreatitis.37 The recent increase use of newly designed core biopsy needles may potentially increase the rate of pancreatitis. In a large North American multicenter study using the SharkCore fine needle biopsy (FNB) needle (Medtronic, Dublin, Ireland), the rate of pancreatitis was 2.9% and post-procedure abdominal pain was 2.2%.8 As the authors revealed, this rate was higher than the anticipated rate for EUS FNA of the pancreas (<1%). Because the overall rate of post-EUS FNA pancreatitis is still low in the universe of patients undergoing pancreaticobiliary EUS, we have selected patients at higher risk based on our hypothesis (sample through normal parenchyma or PD) for a prospective study. Our aims were to determine the rate of pancreatitis and evaluate the associated risk factors in patients undergoing EUS FNA through substantial portion of the normal pancreas (≥5 mm) and through the pancreatic duct. The low risk group comprised of patients that were sampled through less than 5 mm of the normal pancreas.
SUBJECTS AND METHODS
Procedures were performed at the Endoscopy suite of the University of Miami Hospital and Clinics by one single endosonographer from 2013 to 2017. All procedures were done under monitored anesthesia care. All patients consented to undergo the endoscopic procedure. Only the 22 gauge Echotip needle (Cook Endoscopy, Winston-Salem, NC, USA) or the 19 gauge Expect needle for FNB (Boston Scientific, Marlborough, MA, USA) were used. All procedures were done using the Olympus curvilinear array echoendoscope (Olympus GF UCT 140 and UCT 160; Olympus America, Melville, NY, USA). Once the best approach to the target lesion was identified, the area was interrogated with color doppler to evaluate for blood vessels in the needle path. The distance from the outer edge of the lesion to the limit of the pancreatic parenchyma at the projected needle path was measured prior to FNA. Patients undergoing FNA or core biopsy of the pancreas were included if the needle traverses ≥5 mm of the normal pancreatic parenchyma or if the needle went into or through the PD (high risk group for pancreatitis). The low risk group (control) was comprised of patients who underwent pancreatic biopsy during the same interval period and were not sampled through PD or less than 5 mm of the pancreatic parenchyma. Solid pancreatic masses were sampled by FNA with rapid on-site examination of slides. If FNA nondiagnostic, core biopsies (FNB) were perform with the 19 gauge Expect needle and 20 mL of negative pressure using the syringe provided in the needle package. The needle was moved to and from three times inside the solid lesion. Pancreatic Rendez-vous procedures or cases of combined EUS/endoscopic retrograde cholangiopancreatography (ERCP) were not included due to the superimposed risk of pancreatitis associated with ERCP. If a patient had sampling from more than one site of the pancreas, only data from the site that met the inclusion criteria (sample through ≥5 mm of normal pancreas) were recorded for analysis. FNA of the pancreatic duct was done only in cases of dilated PD (>5 mm) with no obstructive lesion identified (stone, mass, stricture) to rule out the main duct IPMN. In all those cases, the ampulla was examined endoscopically to rule out tumor or mucin drainage prior to FNA of the main PD. Chronic pancreatitis was diagnosed by EUS using the Rosemont criteria.9
Patients were monitored in the recovery room for one hour, and a follow-up phone call was done by the investigators or experience endoscopy nurse 24–72 hours after the procedure. Moreover, an automated call system contacted all patients and reported the results to the gastroenterology nurse. All patients were informed prior to leaving the endoscopy suite of an increased risk of pancreatitis since the needle traversed the parenchyma. They were instructed to visit the emergency room if severe pain developed. Serum amylase and lipase levels were obtained in patients who complained of severe abdominal pain through the first 24–72 hours. Post-EUS induced pancreatitis was diagnosed by the presence of abdominal pain with an amylase or lipase level higher than three times the normal level within the first 24–72 hours after the procedure. The following patient's baseline characteristics were obtained: demographics, indication of EUS, measurement (millimeters) of parenchyma traversed by needle, area of pancreas sampled, needle gauge and type, number of passes, history of recent acute pancreatitis (<1 year), previous procedure related pancreatitis, presence of chronic pancreatitis by EUS, and post-procedure pain.
1. Statistical analysis
Each EUS procedure was considered a data point. Categorical variables were reported as frequency with percentages, and contiguous variable were reported as the mean. Mann-Whitney test was used to compare the means and Fisher Exact two-tail test used to compare the categorical variables. We calculated the rate of pancreatitis for each patient's characteristic: gender, type of lesion, biopsy site, indication for EUS, and EUS guided biopsy techniques (needle gauge, number of needle passes, depth of sampling, FNA or core). Patients were divided in two groups (pancreatitis and non-pancreatitis groups), and the characteristics of each one was calculated as a percentage of the total number of patients in that group. Factors associated with acute pancreatitis were compared using the Fisher Exact two-tail test for dichotomous variables. A p-value of less than 0.05 was considered statistically significant. This preliminary analysis indicated parameters associated with acute pancreatitis, and logistic regression analysis was performed to determine which factor(s) was/were predictor(s) of pancreatitis post-FNA. The logistic analysis was done using Stata software (Stata Corp LLC, College Station, TX, USA) and online statspage with a p-value produced by SAS ver. 9.1 (SAS Institute, Cary, NC, USA).
RESULTS
Between December 2013 and September 2017, a total of 712 patients underwent pancreatic biopsy; of those, 163 patients (22.8%) met the inclusion criteria for the high-risk group (≥5 mm) and comprised the study population for associated factors with acute pancreatitis. The mean age was 63 years, 82 females, mean number of needle passes was 3.3 (range, 1–7) in patients at risk for pancreatitis (needle advanced through ≥5 mm of normal parenchyma). Nine patients underwent only a core biopsy, ten had combined FNA/core biopsy, and 144 patients had FNA only. Sampling through the head of pancreas was performed in 100 patients (61.3%) and body/tail in 63 patients (38.6%) (Table 1). All 163 patients were successfully followed-up post-procedure. Two patients were admitted for pain control and pancreatitis was ruled out (1.2%, 2/163). Fifteen patients (15/163, 9.2%) who underwent sampling through ≥5 mm of parenchyma or through the PD wall developed pancreatitis post-EUS FNA. Patients who had sampling through <5 mm of the pancreatic parenchyma had a much lower rate of acute pancreatitis. Among the low risk group (<5 mm), eight patients (8/549, 1.45%) required admission post-procedure. Two patients (0.36%) required admission for post-procedure bleeding and five (0.91%) that developed post procedure pain with no pancreatitis. In the low risk group, only one patient with a large pseudopapillary tumor of the body developed pancreatitis after FNA. The rate of pancreatitis was statistically significant between the high risk and low risk groups (9.2%, 15/163 vs. 0.18%, 1/549) (p<0.001; Fisher Exact, two-tailed). Most patients in this study required admission (range, 1–4 days) for a mild attack of pancreatitis, and one patient managed his symptoms with clear liquid diet and analgesia at home.
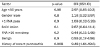
To evaluate other risk factors associated with pancreatitis post-EUS FNA besides sampling through the normal parenchyma, a comparison between patients with and without pancreatitis was analyzed in the 163 patients at risk (Table 1). The rate of pancreatitis by each parameter was also calculated (Table 2). Younger age was more often associated with the outcome of pancreatitis (mean age 49.6 vs. 64.7 years, p=0.01). Patients with a solid lesion had a higher rate of pancreatitis than a cystic lesion (15.7% vs. 3.4%, p=0.01) (Table 2). Moreover, patients who developed pancreatitis were more likely to have a solid lesion than those without (60.0% vs. 32.4%, p=0.04. Fisher Exact test). Recent history of acute pancreatitis was also associated with a higher risk of developing pancreatitis, following EUS-guided biopsy (26.6% vs. 3.3%, p=0.005). The mean number of needle passes was not statistically significant different between the two groups (3.7 pancreatitis vs. 3.2 no pancreatitis, p=0.11, two tailed student's t-test), and also there was no difference between patients who had one single FNA pass compared with more than one pass (5.1% vs. 11.4%, p=0.2). FNA of the pancreatic duct was associated with the highest rate of pancreatitis of all factors analyzed, but it was not statistically significant compared with cysts (17.6% vs. 3.4%, p=0.05; Fisher Exact test), probably due to a small sample size. Although several factors appeared to be associated with pancreatitis post-EUS, logistic regression performed analyzing seven different dichotomous factors (gender male, more than one FNA pass, FNA deeper than 10 mm, solid lesion, age younger than 50 years, benign disease and history of recent acute pancreatitis) demonstrated that only a history of recent acute pancreatitis was a statistically significant predictor (p=0.008) (Table 3).
DISCUSSION
In this study, we have confirmed that the rate of pancreatitis in a subset of patients undergoing biopsy through the normal pancreatic parenchyma or the pancreatic duct is significantly higher than those undergoing FNA through minimal or none of the normal parenchyma (9.2% vs. 0.18%). Our data is in accordance with the results presented by Katanuma et al.4, who in a retrospective study also identified a higher risk of pancreatitis when the needle was advanced through the normal parenchyma. The authors reported that in 73% of patients who had an adverse event (pancreatitis, abdominal pain and bleeding), the needle traversed the normal parenchyma. Univariate analysis indicated that smaller tumors and cases where the needle had to traverse normal parenchyma were strongly associated with post-procedure adverse event.4 In our case, the rate increased, which may be explained by the prospective study design and a very strict follow-up regimen that allowed us to improve the diagnostic rate of acute pancreatitis even beyond the first 24 hours post-procedure. Moreover, pancreatic duct aspiration, which had the highest rate of pancreatitis (17.6%), was done in 17 patients who skewed our rate even higher. Furthermore, the majority of the study population (87.1%) was comprised of benign disease which resulted often sampling through the normal parenchyma at times with multiple biopsies. Patients with malignant disease have a lower rate of pancreatitis after EUS FNA and are under-represented in this group.10
The factors associated with post-procedure pancreatitis in this series were: sampling through the normal pancreatic parenchyma and history of acute pancreatitis. FNA through PD had the highest rate of pancreatitis, but due to small sample size, we could not identify a statistically significant difference. Therefore, based on our collected data to date, we suggest that FNA through PD should be limited and reserved to cases where it will impact clinical decision. After applying a regression analysis for several dichotomous variable, recent history acute pancreatitis was the strongest predictor of post EUS pancreatitis. Other EUS studies have also noted that a recent history of pancreatitis is a predictor of this complication.511 It is recommended that one should wait at least up to 8 weeks for the episode of pancreatitis to resolve prior to FNA.12 However, if one suspects malignancy, waiting eight weeks seems like an unreasonably long time and FNA must be performed sooner, given the increased rate of pancreatitis.
We selected FNA through >5 mm of the normal pancreatic parenchyma as the inclusion criteria for the high-risk group in the current study. In fact, this group had a much higher rate than the control, but when we compared the subgroup with more than 10 mm of needle insertion (78 patients, see Table 1) to less than 10 mm, there was no difference in the rate of pancreatitis. Based on these findings, it seems that pancreatitis after EUS FNA is triggered after trauma to even small amounts of pancreatic parenchyma and may have an individual predisposition. Another interesting finding that corroborates this idea is that we - like other studies - have found no difference in the rate of pancreatitis between the 22 g and 19 g needles.45 We did not use a 25 g needle in this study, but a 19 g was utilized in 19 patients, which should be more traumatic than 22 g; however, no difference was observed. This suggests that a minor trauma with a smaller gauge needle can trigger pancreatitis and that an individual predisposition may be present.
Different from the two prior studies,513 we did not find that pancreatic cysts are associated with higher rate of pancreatitis. Theoretically, patients with a side branch IPMN may have increased risk due to the possibility of FNA causing injury to nearby PD. Siddiqui et al.5 found a six-fold increase in the rate of pancreatitis for IPMN compared to other cysts. We did not separate IPMN from other types of cysts, but patients with cysts had a lower rate of pancreatitis than solid lesions. According to recent American Gastroenterological Association guidelines,14 if only larger cysts (>3 cm) are to undergo FNA, the risk of pancreatitis should be negligible, as in most cases, little normal parenchyma will interpose in the needle path.
Fortunately, all cases of pancreatitis caused by EUS FNA were mild with one of our patients managing to stay home. Most patients were already admitted with a diagnosis of acute pancreatitis by the time of follow-up calls. Three patients developed worsening symptoms only after 24 hours, suggesting that the onset may be a little more insidious than post-ERCP pancreatitis. Understanding post-EUS pancreatitis is important because patients who develop this complication may likely be reluctant to undergo repeated surveillance EUS. Moreover, a physician aware of a prior post-EUS pancreatitis may be more selective in performing FNA. The mechanism of pancreatitis may be related to a focal trauma at the site of needle insertion or injury to PD. It is unclear whether this complication will increase with a newer needle design and more traumatic tip. As aforementioned, a recent FNB needle design SharkCore had a pancreatitis rate of 2.9%, which the authors concluded as slightly higher than historical controls with standard FNA needles.
Our study has some limitations. First, newer needle devices were not used in this study, which would have allowed for better core samples with fewer needles passes potentially decreasing the rate of pancreatitis or may be increasing if newer needles designs lead to more injury to the pancreatic parenchyma. Second, our study included a limited number of patients with malignant disease who have usually a much lower rate of post EUS FNA pancreatitis. Finally, our control group was prospectively obtained from an automated call system, and a GI nurse could have also missed a few cases of pancreatitis; however, this was certainly not to the extent that would significantly increase the rate of pancreatitis in the control group and nullify the difference encountered.
In summary, patients with a history of recent acute pancreatitis undergoing EUS FNA through 5 mm or more of the normal pancreatic parenchyma are at an increased risk of post-EUS FNA pancreatitis. In such cases, an alternative diagnostic method should be considered. We are currently evaluating whether indomethacin suppository may ben beneficial to this particular group in the prevention of acute pancreatitis post-EUS FNA.


 XML Download
XML Download