

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiovascular diseases are the leading cause of mortality. The major direct cause of deaths in 2008 was cardiovascular diseases such as ischemic heart disease, stroke or other forms of cerebrovascular disease [1]. Atherosclerosis is the primary cause of cardiovascular disease, including coronary sclerosis and cerebrovascular disease and is unequivocally an inflammatory disease [2,3]. In clinical studies, blood inflammatory markers such as C-reactive protein (CRP), tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β) and IL-6 are altered during the progression of cardiovascular diseases including coronary sclerosis [4,5]. Additionally, the inflammatory blood vessel response leads to endothelial dysfunction, which is highly relevant to blood vessel diseases such as atherosclerosis and hypertension [3]. Therefore, the blood vessel inflammatory response should be considered in the development of cardiovascular disease.
Cranberry (Vaccinium macrocarpon Ait.) is a fruit rich in polyphenols and flavonoids mainly produced in North America [6]. Cranberry has anti-bacteriuria and anti-pyuria [6,7], antioxidant [8], anti-carcinogenic effects [9], and positive effects on periodontal health [10]. Furthermore, cranberry contributes to reducing the risk for cardiovascular diseases by decreasing low density lipoprotein (LDL) oxidation, inhibiting platelet aggregation, and suppressing blood pressure [11]. Ruel and Couillard [12] suggested the importance of consuming cranberry to maintain health and prevent cardiovascular diseases. Neto [13] also reported that cranberry has the potential ability to limit the progression of various vascular diseases such as atherosclerosis, ischemic stroke, and neurodegenerative diseases through the anti-oxidative and inflammatory effects of the phytochemicals in cranberry. However, cranberry research is still inadequate and has focused mainly on the antioxidant properties and use for urinary tract infections. Only a few studies have investigated the effects of cranberry on cardiovascular diseases, particularly as they relate to the inflammatory response. Additionally, most studies on cranberry utilized cranberry extracts or juices. However, Vinson et al. [14] reported the total phenol content to be higher in dried or frozen cranberry products than that in juice. Therefore, we used freeze-dried cranberry powder to maximize phenolic content in the test material.
The purpose of this study was to determine the ameliorative effect of cranberry on cardiovascular diseases in relation to the inflammatory system. Therefore, we employed the idea of LPS-induced inflammation [15,16] for animals fed an atherogenic diet [16] to stimulate the early events of atherosclerosis. Then, we examined the effects of the freeze-dried cranberry powder on serum lipids, CRP and various inflammation-related cytokines as markers of cardiovascular disease risk and inflammation when rats were treated with an atherogenic diet and LPS.
Materials and Methods
Animals and diet
Forty Sprague-Dawley male rats aged 6-weeks and weighing 160-169 g were obtained from Animals Inc. (Central Lab., Seoul, South Korea) and kept under specific conditions in a temperature (23 ± 2℃) and humidity (50 ± 10%) controlled environment. After 7 days of acclimation, the animals were divided into five groups of similar mean body mass (Fig. 1); one group was provided a normal diet of 5% corn oil (control group, n = 8), two atherogenic diet groups were fed a diet containing 5% corn oil, 10% lard, 1% cholesterol and 0.5% bile acid (HFC, n = 8; HL, n = 8), one group was fed the atherogenic diet with 5% added cranberry powder (HL-C5, n = 8), and one group was fed the atherogenic diet with 10% added cranberry powder (HL-C10, n = 8).
Freeze-dried cranberry powder was purchased from Finlandia (Kiantama Oy Co., Suomussalmi, Finland) and all diet schemes were according to the modified AIN-76 [17] (Table 1). The experimental diets and water were provided ad libitum for 6 weeks. The amount of food consumed was recorded every day, and the animals were weighed weekly.
The NC and HFC groups received 0.9% normal saline injections into the abdominal cavity 18 hours prior to sacrifice, and the HL, HL-C5, and HL-C10 groups had LPS (0.5 mg/kg LPS from Escherichia coli 026:B6, Sigma Co., St. Louis, MO, USA) injected into the abdominal cavity. The animals were sacrificed under ethyl ether anesthesia after a 12-hour fast. Liver and blood samples from the abdominal vein were collected into gel tubes containing coagulant for lipid profiling and biochemical analyses. All blood samples were immediately centrifuged (Sorvall ST16R Centrifuge, Thermo Scientific Co., Rockford, IL, USA) at 3000 rpm and 4℃ for 20 minutes to separate the serum, and stored at -75℃ before analysis.
Total phenolic and total flavonoid assay
According to the method of Ainsworth and Gillespie [18], total soluble phenolic compounds were determined in cranberry powder with the Folin-Ciocalteu reagent using gallic acid as the standard. Distilled water (865 µl) and 50 µl of sample (100 mg freeze-dried cranberry powder in 1 ml distilled water) were incubated with 75 µl Folin-Ciocalteu reagent at room temperature for 5 min. Na2CO3 (225 µl of 20%) and 285 µl of distilled water were added to the reaction mixture, which was incubated at room temperature for 2 hours, and the absorbance was obtained at 760 nm. Total phenolic content is expressed as gallic acid equivalent (GAE) in milligrams per gram of dried sample.
The total flavonoid level in freeze-dried cranberry powder was measured by the method of Jia et al. [19]. Sample (500 µl total) was diluted with distilled water and 75 µl of 5% NaNO2 solution was added and incubated at room temperature for 5 min. This mixture was added to 150 µl of 10% AlCl3, and allowed to stand for a further 5 min before 0.5 ml of 1 M NaOH was added. The solution was measured at an absorbance of 510 nm. The results are presented as catechin equivalents in milligrams per gram of freeze-dried cranberry powder.
Lipid profiles
Serum total cholesterol, HDL-cholesterol, and triglyceride levels were measured with an automatic biochemical analyzer (Vitalab Selectra E, Vital Scientific Co., Dieren, The Netherlands).
Serum CRP and TNF-α
Serum CRP levels were measured with an automatic biochemical analyzer (Vitalab Selectra E).
Serum TNF-α levels were measured with a commercial kit (Rat TNF-α ELISA Kit, Invitrogen Co., Carlsbad, CA, USA) which employs a solid phase sandwich enzyme linked immunosorbent assay (ELISA) technique. Then, optical density was measured at 450 nm with a plate reader (Spectra max 250, Molecular Devices, Sunnyvale, CA, USA).
Serum IL-1β, IL-6, and IL-2
IL-1β and IL-6 contents were measured using corresponding commercial kits (IL-1β: Rat IL-1β ELISA kit, Thermo Scientific, IL-6: Rat IL-6 Immunoassay, R&D Systems Inc., Minneapolis, MN, USA), which employs sandwich ELISA techniques. Optical density values were measured at 450 nm using a plate reader.
IL-2 content was determined with a commercial ELISA kit (Rat IL-2 Immunoassay, R&D System). Optical density values were measured at 450 nm and 540 nm, and then the difference between the 450 nm reading and the 540 nm reading was used for analysis.
Serum IL-10 and NO
Serum IL-10 levels were measured with a commercial ELISA kit (Rat IL-10 ELISA Kit, Invitrogen), and optical density values were read on a plate reader at 450 nm.
NO content was measured using the Griess Reagent System kit (Promega Co., Madison, WI, USA) which employs sulfanilamide and N-1-napthylethylenediamine dihydrochloride under acidic (phosphoric acid) conditions. The serum sample was reacted with the Griess Reagent for 10 minutes, and then absorbance was measured at 520 nm with a plate reader.
Statistical analysis
Statistics were conducted with SAS program version 9.1 (SAS Inc., Cary, NC, USA). Significant differences between groups were evaluated with a one-way analysis of variance and Duncan's multiple range tests. Values are presented as mean ± standard deviation, and P < 0.05 was considered statistically significant.
Results
Total phenolic compounds and total flavonoid levels
The levels of total phenolic and total flavonoid compounds in freeze-dried cranberry powder are shown in Table 2. The total phenolic compound level was 18.17 mg GAE/g, and the total flavonoid level was 7.33 mg catechin equivalents/g.
Body weights and food intake
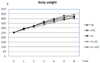
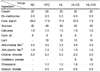
Final body weights and food intakes are shown in Table 3, and changes in body weight are shown in Fig. 2. Mean weights increased gradually in all groups. Food intake in the HFC and HL-C5 groups decreased significantly and that of the other altherogenic diet groups (HL and HL-C10) tended to decrease when compared to food intake in the NC group. In addition, no significant changes were observed in the mean body weights of the groups regardless of altherogenic diet, LPS injection, or cranberry powder treatment.
All atherogenic diet groups displayed a significant increase in liver weights and relative liver weights compared to those in the NC group. Compared to the HFC group, liver weights tended to increase in all groups injected with LPS (HL, HL-C5, and HL-C10) without significant differences (Table 3).
Lipid profiles
The effects of the cranberry powder on serum lipid profiles are summarized in Table 4. Average serum triglyceride level in the NC group was significantly higher than that in the HFC group, and there was a tendency for increased triglycerides in the LPS injected and cranberry powder treated groups. Serum total cholesterol levels in all atherogenic diet groups were significantly higher than those in NC group, but no significant changes were observed in the LPS injection or cranberry treated groups. HDL-cholesterol levels decreased significantly in rats fed the atherogenic diet, but increased with cranberry treatment. The HDL-cholesterol level of the HL-C5 group (63.6 mg/dl) was significantly higher than that of the HFC group (44.9 mg/dl) and HL group (43.2 mg/dl) but was not significantly different from the normal diet group (Table 4).
CRP and TNF-α
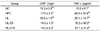
A significant increase in CRP levels was observed in the HFC group compared to those in the NC group. The cranberry diet groups (HL-C5: 14.0 mg/l, HL-C10: 14.2 mg/l) displayed a significant decrease in CRP levels compared to those in the HFC (17.6 mg/l) and HL groups (16.6 mg/l). The CRP levels in the cranberry diet groups were similar or tended to be lower than those measured in the NC group (Table 5).
Serum TNF-α level increased significantly in rats fed the atherogenic diet and cranberry treatment. The HFC group showed a significantly higher mean TNF-α (46.8 pg/ml) level compared to that in NC group (15.2 pg/ml). Additionally, both the HL-C5 (70.3 pg/ml) and HL-C10 groups (57.1 pg/ml) had elevated TNF-α compared to that in the HL group (26.1 pg/ml) (Table 5).
Serum IL-1β, IL-6, and IL-2
Mean serum IL-1β level tended to decrease in rats fed the atherogenic diet, but was elevated by LPS injection. The cranberry diet groups (HL-C5 and HL-C10) displayed a significant decrease in IL-1β levels compared to those in the NC and HL groups (Table 6).
The IL-6 level in the HFC group was significantly lower than that in the LPS injected groups, particularly the HL and HL-C5 groups. Cranberry treatment tended to produce lower IL-6 levels (Table 6).
Mean IL-2 level tended to increase following the LPS injection and significantly increased with the 5% cranberry treatment. The mean IL-2 level in the HL-C5 group was significantly higher than that in the NC, HFC, and HL groups (Table 6).
Serum IL-10 and NO
The mean IL-10 levels in the cranberry diet groups (HL-C5 and HL-C10) were significantly higher than those in the NC and HFC groups. Cranberry treatment tended to increase serum IL-10 levels, but this did not reach significance (Table 7).
Serum NO and IL-10 levels are involved in atherosclerosis through the effect on endothelium-dependent vasodilation, and were measured as an indicator of this effect. Although no significant difference was observed between the groups, the cranberry treated groups (HL-C5 and HL-C10) displayed 88 and 24% increases in NO levels.
Correlation among serum lipids and inflammatory markers
HDL was significantly negatively correlated with serum CRP and total cholesterol. CRP was also negatively correlated with IL-10 and NO levels. Serum TNF-α was significantly positively correlated with total cholesterol, IL-10, and IL-2, but negatively correlated with IL-1β. Additionally, NO was positively correlated with triglycerides and total cholesterol (Table 8).
Discussion
This study was conducted to determine the anti-inflammatory and ameliorative effects of freeze-dried cranberry powder on cardiovascular diseases in relation to the inflammatory system. We investigated serum lipid profiles, CRP, and markers of the inflammatory response related to cardiovascular disease risk in rats fed an atherogenic diet with inflammation-induced by an LPS injection.
Cranberry, one of the flavonoid and polyphenol rich fruits, has beneficial health effects on cancers and vascular diseases [13]. Vinson et al. [14] reported that the average total phenol content was 870 mg/100 g dried cranberries, and it was highest in the freeze-dried product among the fruits tested such as apricots, figs, grapes, raisins, and dried plums. In our previous study, total flavonoid content of freeze-dried cranberry powder was 8.2 mg catechin equivalents/g and total phenolic content was 9.94 mg GAE/g [8]. The freeze dried cranberry powder used in the current study contained about twice the total phenolics than we used in our previous study [8], suggesting that freeze-dried cranberry powder is certainly high in phenolics but that total phenolic content may vary due to the manufacturing process, cranberry type, or maturation stages.
Ryu and Cha [20] have demonstrated that increased carbohydrates in the diet may raise serum triglycerides due to synthesis of hepatic triglycerides. The normal diet used in the current study had a relatively higher composition of carbohydrates than that in the atherogenic diet, and the average food intake in the NC group was significantly higher than that in the other groups. These dietary differences might partially explain the reason why we observed a significantly higher serum triglyceride level in the NC group. In addition, as Uchiumi et al. [21] reported that LPS increases serum triglycerides, we also observed a slight elevation in serum triglycerides following the LPS injection. However, we failed to observe the hypolipidemic effect of cranberry powder. Cranberry improves dyslipidemia in animals and human [2,22]. Ruel et al. [22] reported that cranberry consumption in men resulted in an increase in HDL-cholesterol but no change in total cholesterol. In contrast, Reed [2] reported that cranberry juice powder has the potential to decrease blood total cholesterol levels in an atherosclerotic animal model. Kalgaonkar et al. [23] suggested that total cholesterol, LDL-cholesterol, and LDL oxidation decreased by consuming large amounts of cranberries. Ruel et al. [22] demonstrated increased HDL-cholesterol levels in overweight men after 12 weeks of low-calorie cranberry juice consumption. However, our previous study [8] demonstrated no significant changes in both triglyceride and total cholesterol levels in rats treated with freeze-dried cranberry powder, whereas HDL-cholesterol levels increased significantly with 5% cranberry supplementation. The current study showed similar results regarding the effect of cranberry on serum lipids. The 5% cranberry powder supplementation resulted in a significant increase in HDL-cholesterol levels compared to those in the HL group. Additionally, 10% cranberry powder supplementation displayed a trend towards an increase.
According to the study by Ridker [24], CRP is regarded as an inflammatory indicator and a potential risk factor for cardiovascular disease. CRP facilitates atherosclerosis through influences on vascular cell activation, monocyte recruitment, lipid accumulation, and blood clot formation [25]. Other studies have reported that CRP is an independent risk factor for atherosclerosis, cardiovascular events, and myocardial infarction [26,27]. In the current study, serum CRP levels were significantly elevated in rats on the atherogenic diet for 6 weeks. However, when freeze-dried cranberry powder was added to the diet, the increased CRP decreased significantly to a level even lower than that in rats fed the normal diet. In a population based study, total flavonoid intake was significantly negatively correlated with serum CRP levels in US adults [28]. Chun et al. [28] suggested that flavonoids might inhibit the synthesis and expression of NF-kB, which can influence CRP production as an upstream regulator of pro-inflammatory cytokines synthesis. This might partially explain the effect of flavonoid-rich cranberry on lowering CRP. We observed a significant negative correlation between CRP and HDL-cholesterol. Fröhlich et al. [29] also reported a negative correlation between CRP and HDL-cholesterol in a population based study. It has been suggested that HDL is a potential anti-inflammatory particle because of the antiinflammatory effect of Apo A1, which is a major HDL protein [12].
IL-1β and IL-6, inflammation-mediatory cytokines, play important roles in vascular inflammation and progression of atherosclerosis [30]. IL-1β induces necrosis and infection by causing damage to blood vessels [31], and IL-6 is a potent stimulant of CRP generation in the liver [32]. Huang et al. [6] reported a significant decrease in LPS-induced IL-1β production in human peripheral blood mononuclear cells after treatment with cranberry extract. Bodet et al. [33] mentioned that macrophage production of pro-inflammatory cytokines including IL-1β and IL-6 are inhibited by the highly concentrated proanthocyanidin fraction of a cranberry extract. Our results showed that serum IL-1β and IL-6 levels increased following an LPS injection and decreased with cranberry powder treatment, particularly the 10% cranberry powder supplement. Reed [2] and Park et al. [34] suggested that flavonoids inhibit the production of inflammatory cytokines such as IL-6 and IL-1β by acting as gene expression inhibitors and the production of pro-inflammatory cytokines by suppressing activation of transcription factors such as NF-kB and NF-kB/DNA binding. TNF-α is an indicator of the systemic inflammatory response related to atherosclerosis and cause the expression of endothelial cell adhesion factors [35]. In human studies, serum TNF-α level increases in patients with coronary artery disease and secretion of TNF-α by mononuclear leukocytes increases in patients with ischemic heart disease [36]. Additionally, Bodet et al. [33] reported decreased TNF-α secretion by LPS-induced macrophages following treatment with a high-molecular-weight cranberry fraction from cranberry juice, which contained mainly anthocyanins and proanthocyanidins at levels 125 times higher than those in freeze-dried cranberry juice. Bodet et al. [33] assumed that the effects were due to concentration of active compounds including proanthocyanidins in the high-molecular-weight cranberry fraction. In contrast, TNF-α production in LPS-stimulated human leukemia cells increases when cells are treated with a cranberry polyphenol fraction, although NF-kB activation is down-regulated by cranberry polyphenols [37]. Similarly, we observed noticeable elevations in serum TNF-α levels in the groups fed cranberry, suggesting that TNF-α expression may be up-regulated by alternate pathway other than NF-kB [38].
IL-2 may promote expansion and activation of Th1 cells, causing plaque development, which is believed to actively promote atherogenesis [39]. Nabata et al. [40] suggested that IL-2 is related to the pathogenesis of atherosclerosis and vascular disease by modulating the response to angiotensin II. Procyanidins, abundant in cranberry and chocolate, inhibit IL-2 expression and modulate IL-2 production in cells [41]. However, in the current study, we failed to define any noticeable modulatory effect of cranberry powder on IL-2 levels.
IL-10 is a well known anti-inflammatory cytokine, which has anti-atherogenic and anti-apoptotic properties [42]. While IL-10 production is increased by polyphenols [43], IL-10 is regulated by the production of pro-inflammatory cytokines such as IL-1β, IL-6, and TNF-α in infection or tissue damage [44]. In the current study, we found a significant positive correlation between IL-10 and TNF-α. In addition, Lakoski et al. [45] reported that elevated IL-10 level is related with a risk for cardiovascular heart disease events and suggested that IL-10 might increase by the response to the pro-inflammatory environment of atherosclerosis. In a study by Deitschel et al. [46], IL-10 production was stimulated by LPS treatment in dogs. Similarly, we observed a tendency for increasing IL-10 levels in the LPS injected group compared to those in the non-LPS injected group. While we assumed that this increase was a response to the induction of an inflammatory reaction to LPS, there were further enhancements of IL-10 levels observed in rats fed the cranberry powder supplement. These results suggest that IL-10 production might be boosted by cranberry powder treatment during the inflammatory reaction induced by LPS. Similarly, Svajger et al. [43] demonstrated that the polyphenol resveratrol increases IL-10 production from LPS-treated dendritic cells. However, the mechanism of IL-10 increasing effect of polyphenols or polyphenol rich food products needs to be further elucidated.
NO plays an important role in vascular endothelial cell function. It inhibits a rise in blood pressure and has a vasodilatory effect [47]. NO is produced by the enzyme nitrogen oxide synthase (NOS) acting on L-arginine, and acts as an antioxidant via diffusion. NO protects LDL against oxidation, inhibits platelet aggregation, and decreases endothelial adhesion of leukocytes [23]. However, Huang et al. [6] reported no significant effect of cranberry extract on the activity of NOS in vivo. In contrast, we found that cranberry powder fortified groups showed an increasing trend in NO levels, although it did not reach significance. Similarly, proanthocyanins have been demonstrated to increase endothelial NO production and improve vasodilation in an in vitro experiment [48]. Maher et al. [49] reported that phenolics from cranberry juice have an NO-dependent vasodilation and blood pressure decreasing effect in rats, suggesting that NO might have potential roles as an antioxidant or vasodilator in vascular endothelial cells helping to stabilize cardiovascular diseases.
In summary, when 5 or 10% cranberry powder was supplemented with a high fat diet, LPS-treated rats seemed to achieve some anti-inflammatory effects by reducing serum CRP, IL-1β and IL-6, and enhancing IL-10 in dose-dependent manner. Similar to previous reports, consuming cranberry products might also have potential cardiovascular benefits possibly by modifying serum lipids and biomarkers of inflammation [11,12,22,33]. However, we observed an increased TNF-α level when cranberry powder was supplemented with the diet. Additionally, there is no consensus among studies for the effect of cranberry on TNF-α production [33,37]. Therefore, various bioactive components of cranberry need to be classified and tested to better understand the function of cranberry as an inflammation regulator. Furthermore, transcriptional mechanisms of action for the cranberry flavonoids should be verified in relation to their function of modifying biomarkers of inflammation.







 XML Download
XML Download