

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With the remarkable advancement of modern medicine as well as economic development, human longevity and the prevalence of chronic diseases due to the aging process have increased. Osteoporosis is one representative disease that occurs in the elderly, and according to the Korean National Health and Nutrition Examination Survey in 2008, prevalence rates of osteoporosis and osteopenia were reported as 32.6% and 45.5%, respectively, in women aged 50 years or older [1]. It is therefore essential to prevent the occurrence of bone fractures and osteoporosis, among which incidence rates have abruptly increased in middle-aged and elderly individuals, by maintaining a healthy skeletal structure during the 20s, the time when maximal bone mass is achieved [2].
However, in an environment where slender women are favored from a social perspective, bone mineral density has been contradictorily reported to be lower in women in their 20s who are highly interested in body weight control as compared to those in their 30s [3]. It is therefore imperative that young women secure maximal bone mass through healthy dietary habits and living habits [4]. Factors affecting bone mineral density include the following: age of menarche [5], body weight, amount of muscle, BMI [6], smoking [7], estrogen and progesterone status [8], and dietary intakes of vitamin D [9], isoflavones [10] and vitamin K [11]. Particularly in association with bone metabolism, vitamin K plays an essential role as a coenzyme during the carboxylation of γ-glutamic acid within the protein osteocalcin [12]. Carboxylated osteocalcin binds to hydroxyapatite and is thereby involved in bone formation. Serum osteocalcin is used as a bone metabolism marker that is associated with the homeostasis of bone formation [13].
The percentage of undercarboxylated osteocalcin (%ucOC) is referred to as the ratio of osteocalcin released to the peripheral blood in a non-carboxylated state, and it has a negative correlation with vitamin K nutritional status [14]. It is therefore used as a sensitive marker of bone metabolism in association with vitamin K deficiency [15,16].
According to studies on correlations between vitamin K and bone mineral density, there was a positive correlation between vitamin K intake level and bone mineral density and a negative correlation with incidence of pelvic bone fracture in women [17,18]. In addition, it was also been reported that %ucOC decreased following supplementation of vitamin K1 in adult women in their 20s [19]. According to animal experiments, supplemental vitamin K suppressed the formation of osteoclasts and facilitated apoptosis in rats. This eventually led to decreased occurrence of bone loss [20]. To explain the mechanisms by which vitamin K is involved in bone metabolism, its relationship with cytokines as well as action as a coenzyme have been proposed. According to the Framingham Offspring Cohort cross-sectional study, following the measurement of vitamin K levels in subjects in a community-based setting, proinflammatory cytokines such as IL-6, intercellular adhesion molecule-1 (ICAM-1), and tumor necrosis factor receptor 2 (TNFR2) were found to be negatively correlated with vitamin K [21]. Furthermore, according to Shea et al. [22], the concentration of serum high sensitivity C-reactive protein (hs-CRP), a sensitive inflammatory marker, had a negative correlation with serum vitamin K concentration. Moreover, according to a cross-sectional study conducted in elderly individuals, there was a positive correlation between osteoprotegerin, an inflammatory marker suppressing bone loss reactions, and vitamin K. This implies that vitamin K is involved in inflammatory responses associated with bone metabolism. In Korea, however, there are still an insufficient number of studies on the relationship between vitamin K nutritional status, inflammation indicators, and bone mineral density.
Given the above background, we examined the relationships between %ucOC, hs-CRP (a proinflammatory marker), and bone mineral density in women in their 20s in whom maximal bone mass is formed. Thus, we attempted to provide baseline data for nutritional education on the maintenance of bone health in order to prevent osteoporosis in women.
Subjects and Methods
Subjects
The current study was approved by the Institutional Review Board (IRB) of Wonkwang University Hospital, and was conducted in women in their 20s from July to September of 2009. Of the 86 subjects who submitted a written informed consent, 11 had study data that were incompletely collected. Seventy-five subjects were finally enrolled in the current study.
Methods
Physical examination
The height and weight of subjects were measured using an automatic measurer, a DS-102 (Jenix Co, Korea). Body mass index (BMI), body fat amount, and its percentage were measured using an Inbody 3.0 (Biospace Co, Korea), for which the subjects wore minimal clothing by taking off their shoes and socks and removing metal items.
Measurement of bone mineral density
To measure bone mineral density, an Osteo pro smart (Bio medical technology Co, Korea) device, which is an automatic measurer of bone mineral density, was used. Bone mineral density was measured by a quantitative ultrasonographic method based on decreased velocity of ultrasound that passes bone tissue. Data such as height, weight, date of birth, sex, and foot size were entered for the measurement of bone mineral density. In terms of body positioning, the knees were bent at a right angle in a sitting position and then the right ankle was measured in such a condition that the calf and foot formed a right angle.
Biochemical assay
Venous blood samples were taken from the subjects after more than a 12-hr fasting state. The samples were centrifuged and the serum was isolated accordingly. Blood glucose, total cholesterol, triglyceride (TG), total protein (TP), and albumin were measured using a Mindray BS-220 (Mindray, China).
Measurements of serum osteocalcin and undercarboxylated osteocalcin
The concentrations of osteocalcin and undercarboxylated osteocalcin (ucOC) in the serum were measured using a Takar kit and an Elisa Reader (Molecular Devices, USA). Percent ucOC was also calculated as shown below:

The %ucOC was analyzed based on tertiles. In each group, the first, second, and third teritiles of %ucOC were < 19.34%, 19.34-32.01%, and > 32.01%, respectively.
Measurement of serum hs-CRP
hs-CRP was measured using a Hitachi 7600-110 (Hitachi, Japan) based on optical density methods with Pureauto S CRP Latex.
Dietary assessment
Evaluations of food intake were performed via interviews by investigators who had been trained on the 24-hr recall method. To accurately determine food intake, amounts were estimated by eye measurements using food models. All analyses were performed using Can-pro 3.0; a computer-aided nutritional analysis software program developed by the Korean Nutrition Society. For the food database of vitamin K, a pre-existing database was combined with that of the Rural Development Administration [23] and the USDA National Nutrient Database [24]. The standard guidelines for energy and nutrient intakes were based on estimated energy requirements (EER), estimated average requirements (EAR), and adequate intakes (AI). The percentages of recommended intake were analyzed to assess nutritional quality [25].
Statistical analysis
Statistical analyses were performed using SPSS (Statistical Package for Social Science) 12.0. Measurements are expressed as the mean and SD (standard deviation). ANOVA was performed to assess statistical significance depending on %ucOC between the three groups. For an inter-group analysis, a post-hoc analysis was performed with Tukey's test. Multiple regression analysis was used to assess associations between biochemical indicators (serum %ucOC, cholesterol, and triglycerides) and the inflammatory marker hs-CRP, as well as the status of bone mineral density. The covariates that were considered in these models included age and body mass index (BMI). Statistical significance was set at P < 0.05.
Results
General characteristics and physical examination
Based on tertiles of %ucOC, the subjects' general characteristics and physical examination findings were analyzed. The results are presented in Table 1. Between the three groups, there were no significant differences in age, height, amount of muscle, amount of body fat, waist to hip ratio, percentage of body fat, or BMI. Mean BMI was measured as 21.18 ± 2.37 kg/m2, which was within the normal range [26].
Analysis of bone mineral density
The results for bone mineral density measurements are presented in Table 2. The T-scores for the first and third tertiles were 1.06 and -0.03, respectively. These results indicate that T-scores were significantly lower as %ucOC values increased (P < 0.05). In the group where %ucOC values corresponded to the highest tertiles, Z-scores, OI (Osteoporosis index), and SOS (Speed of sound) were significantly lower as compared to %ucOC values corresponding to the lowest tertiles (P < 0.05).
Biochemical assessment
Blood glucose, total cholesterol, triglycerides, total protein, and albumin were measured in the study subjects and the results are presented in Table 3. The first, second, and third tertiles of blood glucose were 91.00 ± 7.02 mg/dl, 94.42 ± 5.83 mg/dl, and 90.20 ± 6.09 mg/dl (P < 0.05), respectively, and were in normal range. There were no significant differences in total cholesterol, triglyceride, total protein, and albumin between the three groups. Concentrations of osteocalcin and non-carboxylated osteocalcin were 17.52 ± 5.14 ng/ml and 2.52 ± 0.73 ng/ml in the highest tertile group, and 8.10 ± 5.28 ng/ml and 4.39 ± 3.35 ng/ml in the lowest tertile group, respectively, and there were significant difference between the groups (P < 0.001, P < 0.01). Tertile values of serum hs-CRP showed an increasing tendency as values of %ucOC increased; the first, second, and third tertiles of serum hs-CRP were 0.04 ± 0.02 mg/dl, 0.07 ± 0.04 mg/dl, and 0.11 ± 0.18 mg/dl, respectively, but these were not statistically significant.
Assessment of daily intake
Inter-group comparisons of nutrient intake amounts depending on values of %ucOC are presented in Table 4. Calorie intake and protein intake were found to be highest in the group where values of %ucOC were lowest. The first, second, and third tertile values of daily vitamin K intake were measured as 94.88 ± 51.48 µg, 73.85 ± 45.15 µg, and 62.58 ± 39.92 µg, respectively, and were significantly different (P < 0.05). There were also significant differences in intake amounts of nutrients such as iron, phosphorus, zinc, and vitamin B6 between the classified groups based on values of %ucOC (P < 0.05). Following the calculations of percentages of recommended nutrient intakes, all study subjects were found to have intakes of protein, phosphorus, vitamin A, vitamin B2, niacin, vitamin B6, and vitamin B1 that were greater than the recommendations. As compared to the recommendations, however, all the study subjects consumed insufficient amounts of calcium, folic acid, and vitamin C.
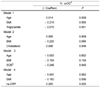
Correlations between serum %ucOC, inflammatory markers, and bone mineral density
We examined the relationships between %ucOC, biochemical markers, and bone mineral density, and the results are presented in Table 5. There was no association between serum %ucOC and serum triglycerides or between serum %ucOC and cholesterol, after adjusting for covariates. There was a negative correlation between serum %ucOC and hs-CRP. However, there was a positive correlation between serum %ucOC and bone mineral density, which was measured by an ultrasonographic method.
Discussion
We examined concentrations of serum hs-CRP, an inflammatory marker, along with bone mineral density and vitamin K nutritional status in young women in their 20s. Then, we also examined the relationships between these parameters. The 20s is the period of age in which bone mass reaches a maximum. During this period, bone health and nutritional status are important to prevent osteoporosis during the elderly years [27]. In the current study, the mean T-score of the study subjects was 0.38. In particular, in the group with the highest %ucOC and where the degree of vitamin K nutritional status was relatively lower, the T-score was measured as -0.03. This value corresponded to the normal range according to WHO criteria. It is presumed, however, that further risks of developing osteopenia would increase considering that the enrolled subjects were women in their 20s who maintained a maximal degree of bone mass.
As a marker indicating bone formation, osteocalcin is a bone-specific protein composed of 49 amino acids. It is also one of the non-collagen proteins forming bone matrix, which is used as a marker to predict degree of bone formation [28-30]. In regard to the concentration of serum osteocalcin, following the synthesis of osteocalcin in osteoblasts, osteocalcin accumulates in the bone matrix and its residual amount is measured following its release into the blood. Accordingly, an increased concentration of serum osteocalcin is indicative of increased bone formation [31]. In our study, the mean concentration of serum osteocalcin was 12.06 ng/ml. This value was relatively higher than 11.8 ng/ml, as measured by Hong [32] in postmenopausal women, and 8.30 ng/ml as measured by Sung et al. [33]. These results indicate that degrees of bone formation are relatively higher in younger women.
In association with the maintenance of a healthy skeletal structure, protein plays a key role in forming and then maintaining maximal bone mass. Yet, excessive intake of animal protein decreases calcium absorption from the kidneys and this has a detrimental effect on the formation of skeletal structure [34]. In this study, when compared with the EAR for protein (35 g), the subjects were found to have a protein intake ratio of 155.48%. Intake amounts of essential nutrients for the formation of skeletal structure, including calcium, zinc, folic acid, and vitamin C, were all found to be insufficient as compared to their EAR values. In particular, in the group where %ucOC was highest, degrees of nutrient insufficiency were also found to be relatively higher. Accordingly, in women in their 20s, in whom maximal bone mass is reached, an appropriate intake of protein is mandatory. Therefore, these subjects should be instructed to consume vitamins and minerals that might be easily deficient.
In our study, vitamin K was found to be appropriately consumed at an amount of 78.82 µg, as compared to the mean daily AI of 65 µg proposed by the KDRIs. To date, not many studies have been conducted to analyze the status of vitamin K intake in Korea. According to Hong [32] who examined postmenopausal women, vitamin K was found to be consumed at an amount of 379 µg. According to a study conducted to analyze vitamin K intake in young Japanese women, the average intake was 155.9 µg [35], and it was approximately 80 µg in American women under age 45 [36]. In our study, the amount of vitamin K intake was relatively lower than the results of previous studies. This might be due to factors associated with differences in dietary habits between countries, a deficiency of green leafy vegetables containing higher amounts of vitamin K, and lower food intake because of excessive interest in body weight control in younger women.
In such a condition where osteocalcin is not carboxylated due to the depletion of vitamin K, osteocalcin is not effective for bone formation and is released to the blood as a form of ucOC. ucOC has therefore been used as a marker indicating vitamin K nutritional status [37]. In recent years, however, the proportion of uncarboxylated osteocalcin has been measured in proportion to the amount of osteocalcin, and this is referred to as %ucOC. Therefore, %ucOC has been proposed as a more sensitive indicator of vitamin K nutritional status [37]. In the current study, the degree of vitamin K intake was relatively lower in the group where %ucOC was relatively higher as compared to other groups. These results are in agreement with previous reports demonstrating a negative correlation between vitamin K intake and %ucOC [38,39]. However, the young women in the present study had a relatively high degree of undercarboxylated serum osteocalcin (mean 32.5%) than subjects in other studies (21.9% for healthy girls in Denmark [38], 7.5% for healthy adults [19], 13.0% for postmenopausal women in the USA [39]).
According to a cohort study that was conducted to examine the correlation between proximal femur fracture and level of vitamin K intake in the elderly, incidence of fracture was relatively lower in subjects with higher intakes of vitamin K [16,40]. It was also reported that risks of developing hip joint fractures were decreased following the intake of vitamin K [41]. Furthermore, it is recommended that vitamin K should be ingested at an amount of > 500 µg/day for the prevention of bone fractures [42]. In the current study, which was conducted in women in their 20s, there was a negative correlation between %ucOC and bone mineral density, which is in agreement with previous reports that studied elderly patients and patients with bone fractures. Therefore, in women in their 20s during which maximal bone mineral density is reached, special attention should be given to vitamin K intake to ensure adequate stores of the nutrient.
Osteoporosis is a disease occurring as a result of imbalances in bone remodeling due to the predominance of bone resorption over bone formation, during which various key factors are involved in bone physiology and regeneration [43]. Pro-inflammatory cytokines involved in inflammatory responses, such as interleukin (IL)-6 and CRP, have also been revealed to regulate bone metabolism even in healthy individuals without immunological diseases [44]. IL-6 is synthesized from osteoblasts, monocytes, and T-cells and it facilitates the differentiation and activation of osteoclasts [45]. C-reactive protein (CRP) belongs to the pentaxin family of immune-recognition proteins, and it is a sensitive marker for systemic inflammatory responses. Furthermore, it was recognized that IL-1, IL-6, and TNF-α are regulatory factors for the synthesis of CRP [46,47]. According to Bae et al. [48] who examined the correlation between bone mineral density and hs-CRP, as concentrations of serum hs-CRP increased, bone mineral density decreased and bone turnover rate was increased [49]. These authors therefore proposed that serum hs-CRP is closely associated with bone metabolism and inflammatory responses. According to a study on correlations between vitamin K and inflammatory responses, there were positive correlations between %ucOC and two inflammatory markers (IL-6 and hs-CRP). Moreover, in the current study following regression analysis, as values of %ucOC indicating vitamin K deficiency increased, concentrations of serum hs-CRP also significantly increased. Because there remains an insufficient amount of definite data on inflammatory markers and mechanisms associated with vitamin K, further studies are needed.
The limitations of the current study are as follows: The study was a cross-sectional design and it did not clarify whether there are causal relationships between vitamin K nutritional status, bone mineral density, and inflammatory markers. Further studies are therefore warranted to clarify any causal relationships. Nevertheless, the current study is of great significance in that it includes an analysis of correlations between vitamin K nutritional status and inflammatory responses in healthy adult women who had not yet developed specific types of bone disease.




 XML Download
XML Download